

The efficacy and safety of perioperative glucocorticoid for total knee arthroplasty: a systematic review and meta-analysis
- PMID: 38622510
- PMCID: PMC11017604
- DOI: 10.1186/s12871-024-02530-9
The efficacy and safety of perioperative glucocorticoid for total knee arthroplasty: a systematic review and meta-analysis
Abstract
Background: An increasing number of individuals undergo total knee arthroplasty (TKA), which can result in pain, limited motor function and adverse complications such as infection, nausea and vomiting. Glucocorticoids have been shown anti-inflammatory and antiemetic effects, but can also elevate blood glucose levels and increase the risk of wound infection. Thus, it is essential to investigate the efficacy and safety of glucocorticoid usage in TKA.
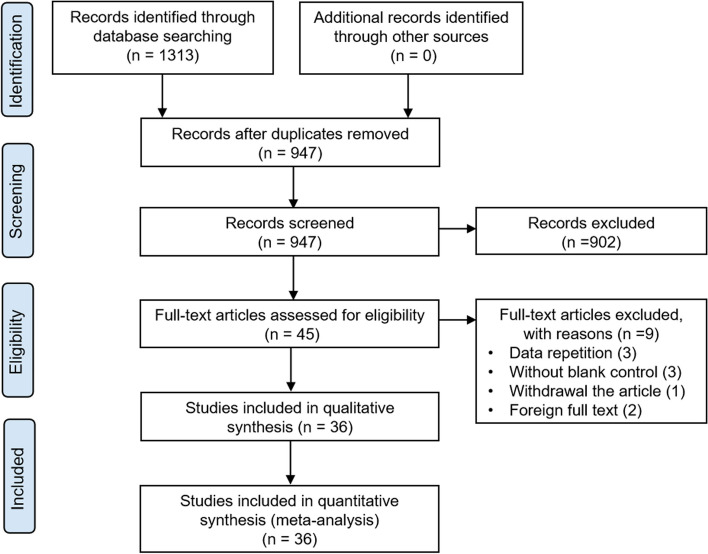
Method: A comprehensive systematic search of PubMed, Medline, EMBASE, Cochrane databases, to identify relevant randomized controlled trials (RCTs) of glucocorticoid application in TKA. The primary outcomes assessed were the postoperative pain assessment. Secondary outcomes included the range of motion in knee joint, levels of inflammatory cytokines, adverse complications, and the length of hospital stay.
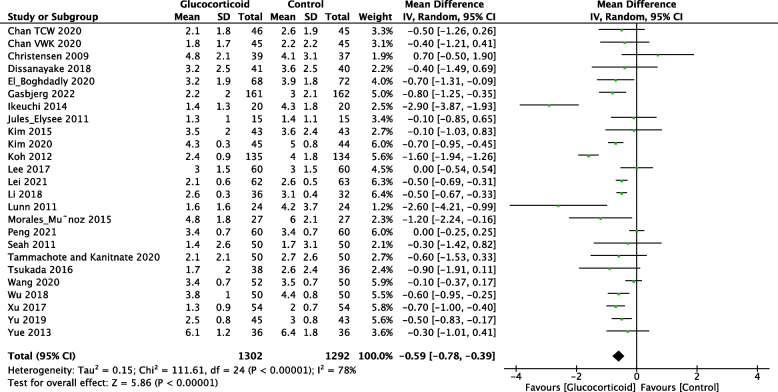
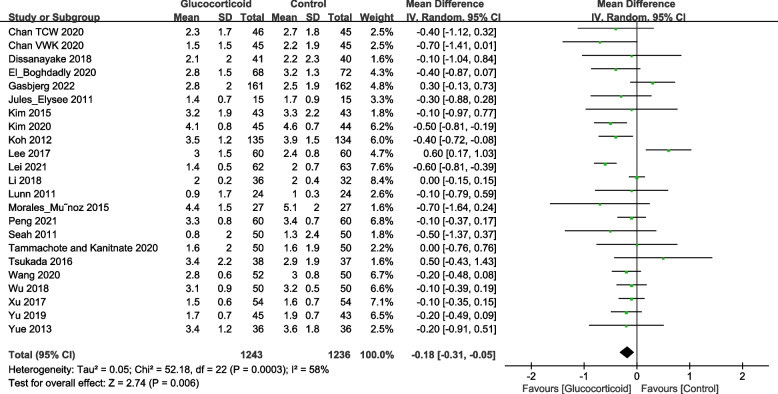
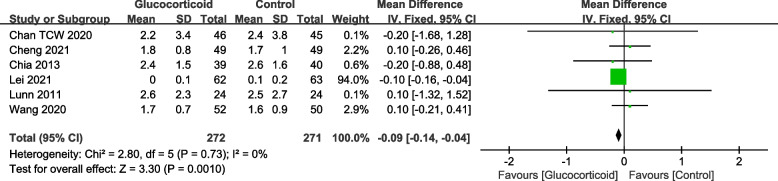
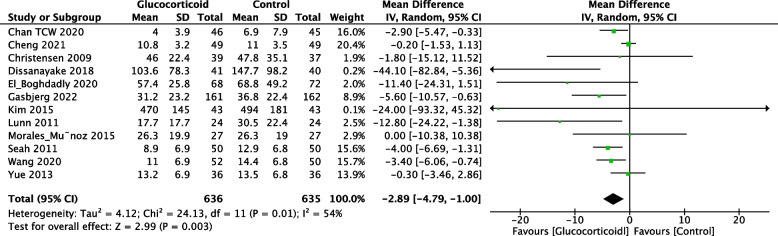
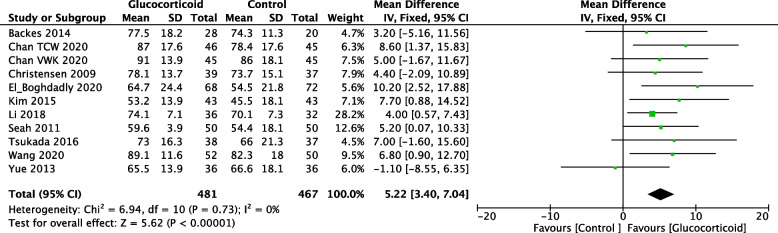
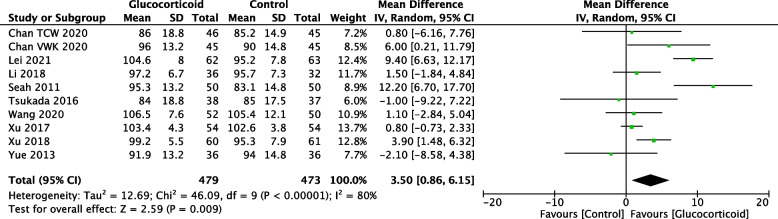
Results: Thirty-six randomized controlled trials were included in the final analysis. The glucocorticoid group exhibited significant reduction in the resting VAS scores on postoperative days 1, 2 (POD1, 2)and postoperative 3 months (POM3), as well as decreased morphine consumption on POD1 and increased range of motion (ROM) in knee joint on POD1, 3. Additionally, the glucocorticoid group exhibited decreased levels of postoperative inflammatory cytokines and the incidence of PONV along with a shorter length of hospital stay. The blood glucose concentration was significantly increased in the glucocorticoid group on POD1 compared with the control group. While the blood glucose on POD2 and occurrence of postoperative adverse complications were similar between two groups including wound infection and venous thrombosis. The periarticular injection analgesia (PIA) group demonstrated lower VAS scores on POD2 comparing to the systemic administration (SA) group according to two studies. However, there was no significant difference of the resting VAS on POD1 and POD2 between PIA and SA group across all studies.
Conclusion: Perioperative glucocorticoids treatment in TKA significantly reduced short-term pain score and opioid-use which was probably not patient relevant. The application of glucocorticoids in TKA implied a beneficial trend in analgesic, anti-inflammatory, and antiemetic effects, as well as improved range of motion and shortened hospital stay. While it will not increase the risk of continued high glucose, postoperative wound infection and venous thrombosis.
Keywords: Glucocorticoid; Inflammation; Meta-analysis; TKA; VAS.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Efficacy of additional corticosteroids to multimodal cocktail periarticular injection in total knee arthroplasty: a meta-analysis of randomized controlled trials.J Orthop Surg Res. 2021 Jan 22;16(1):77. doi: 10.1186/s13018-020-02144-0. J Orthop Surg Res. 2021. PMID: 33482865 Free PMC article.
-
Efficacy of Additional Corticosteroid in a Multimodal Cocktail for Postoperative Analgesia Following Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials.Pain Pract. 2019 Mar;19(3):316-327. doi: 10.1111/papr.12740. Epub 2019 Jan 1. Pain Pract. 2019. PMID: 30354013 Review.
-
The Efficacy and Safety of Glucocorticoid on Periarticular Infiltration Analgesia in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Arthroplasty. 2021 Sep;36(9):3340-3350. doi: 10.1016/j.arth.2021.03.056. Epub 2021 Apr 26. J Arthroplasty. 2021. PMID: 33926778
-
Adding corticosteroids to periarticular infiltration analgesia improves the short-term analgesic effects after total knee arthroplasty: a prospective, double-blind, randomized controlled trial.Knee Surg Sports Traumatol Arthrosc. 2021 Mar;29(3):867-875. doi: 10.1007/s00167-020-06039-9. Epub 2020 May 2. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32361928 Clinical Trial.
-
Effect of Intravenous Dexamethasone on Postoperative Pain in Patients Undergoing Total Knee Arthroplasty: A Systematic Review and Meta-Analysis.Pain Physician. 2022 Mar;25(2):E169-E183. Pain Physician. 2022. PMID: 35322969
Cited by
-
Impact of Dexamethasone on Blood Glucose After Total Knee Arthroplasty in Patients With Type 2 Diabetes.Orthop Surg. 2025 Mar;17(3):814-821. doi: 10.1111/os.14333. Epub 2025 Jan 28. Orthop Surg. 2025. PMID: 39871680 Free PMC article.
-
Comparison of analgesic effects between betamethasone and dexamethasone in total knee arthroplasty: a prospective randomized controlled trial.Front Med (Lausanne). 2025 Jul 9;12:1575417. doi: 10.3389/fmed.2025.1575417. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40703273 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
