

From symptom onset to ED departure: understanding the acute care chain for patients with undifferentiated complaints: a prospective observational study
- PMID: 38622511
- PMCID: PMC11020825
- DOI: 10.1186/s12245-024-00629-x
From symptom onset to ED departure: understanding the acute care chain for patients with undifferentiated complaints: a prospective observational study
Abstract
Background: For most acute conditions, the phase prior to emergency department (ED) arrival is largely unexplored. However, this prehospital phase has proven an important part of the acute care chain (ACC) for specific time-sensitive conditions, such as stroke and myocardial infarction. For patients with undifferentiated complaints, exploration of the prehospital phase of the ACC may also offer a window of opportunity for improvement of care. This study aims to explore the ACC of ED patients with undifferentiated complaints, with specific emphasis on time in ACC and patient experience.
Methods: This Dutch prospective observational study, included all adult (≥ 18 years) ED patients with undifferentiated complaints over a 4-week period. We investigated the patients' journey through the ACC, focusing on time in ACC and patient experience. Additionally, a multivariable linear regression analysis was employed to identify factors independently associated with time in ACC.
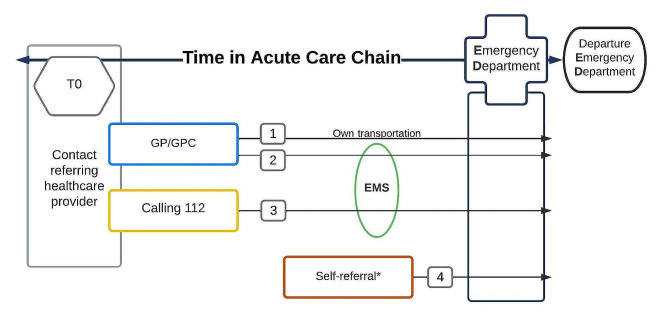
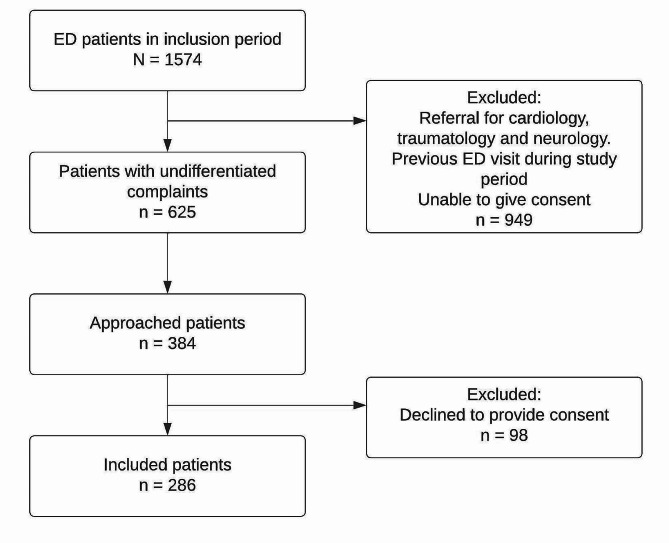
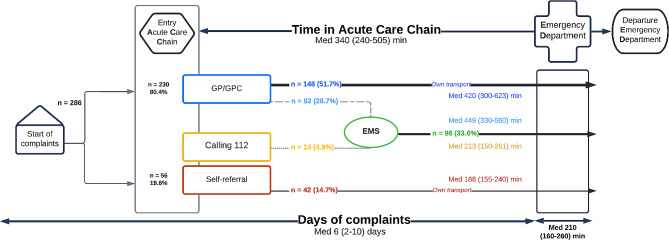
Results: Among the 286 ED patients with undifferentiated complaints, the median symptom duration prior to ED visit was 6 days (IQR 2-10), during which 58.6% of patients had contact with a healthcare provider before referral. General Practitioners (GPs) referred 80.4% of the patients, with the predominant patient journey (51.7%) involving GP referral followed by self-transportation to the ED. The median time in ACC was 5.5 (IQR 4.0-8.4) hours of which 40% was spent before the ED visit. GP referral and referral to pulmonology were associated with a longer time in ACC, while referral during evenings was associated with a shorter time in ACC. Patients scored both quality and duration of the provided care an 8/10.
Conclusion: Dutch ED patients with undifferentiated complaints consulted a healthcare provider in over half of the cases before their ED visit. The median time in ACC is 5.5 h of which 40% is spent in the prehospital phase. Those referred by a GP and to pulmonology had a longer, and those in the evening a shorter time in ACC. The acute care journey starts hours before patients arrive at the ED and 6 days of complaints precede this journey. This timeframe could serve as a window of opportunity to optimise care.
Keywords: Acute care chain; Patient journey; Undifferentiated complaints.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Characteristics of Dutch ED patients and their journey through the acute care chain: A province-wide flash-mob study.PLoS One. 2025 Apr 3;20(4):e0318510. doi: 10.1371/journal.pone.0318510. eCollection 2025. PLoS One. 2025. PMID: 40179077 Free PMC article.
-
Characteristics of the prehospital phase of adult emergency department patients with an infection: A prospective pilot study.PLoS One. 2019 Feb 7;14(2):e0212181. doi: 10.1371/journal.pone.0212181. eCollection 2019. PLoS One. 2019. PMID: 30730990 Free PMC article.
-
Prehospital paths and hospital arrival time of patients with acute coronary syndrome or stroke, a prospective observational study.BMC Emerg Med. 2016 Jan 9;16:3. doi: 10.1186/s12873-015-0065-y. BMC Emerg Med. 2016. PMID: 26748628 Free PMC article.
-
Serum markers in the emergency department diagnosis of acute myocardial infarction.Emerg Med Clin North Am. 2001 May;19(2):321-37. doi: 10.1016/s0733-8627(05)70186-3. Emerg Med Clin North Am. 2001. PMID: 11373981 Review.
-
Characterising patient complaints in out-of-hours general practice: a retrospective cohort study in Ireland.Br J Gen Pract. 2018 Dec;68(677):e860-e868. doi: 10.3399/bjgp18X699965. Epub 2018 Nov 19. Br J Gen Pract. 2018. PMID: 30455221 Free PMC article.
References
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–55. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
-
- Latten G, Hensgens K, de Bont, Eefje GPM, Muris JWM, Cals JWL, Stassen P. How well are sepsis and a sense of urgency documented throughout the acute care chain in the Netherlands? A prospective, observational study. BMJ Open. 2020;10(7):e036276–036276. doi: 10.1136/bmjopen-2019-036276. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
