

The value of admission avoidance: cost-consequence analysis of one-year activity in a consolidated service
- PMID: 38622593
- PMCID: PMC11017527
- DOI: 10.1186/s12962-024-00536-1
The value of admission avoidance: cost-consequence analysis of one-year activity in a consolidated service
Abstract
Background: Many advantages of hospital at home (HaH), as a modality of acute care, have been highlighted, but controversies exist regarding the cost-benefit trade-offs. The objective is to assess health outcomes and analytical costs of hospital avoidance (HaH-HA) in a consolidated service with over ten years of delivery of HaH in Barcelona (Spain).
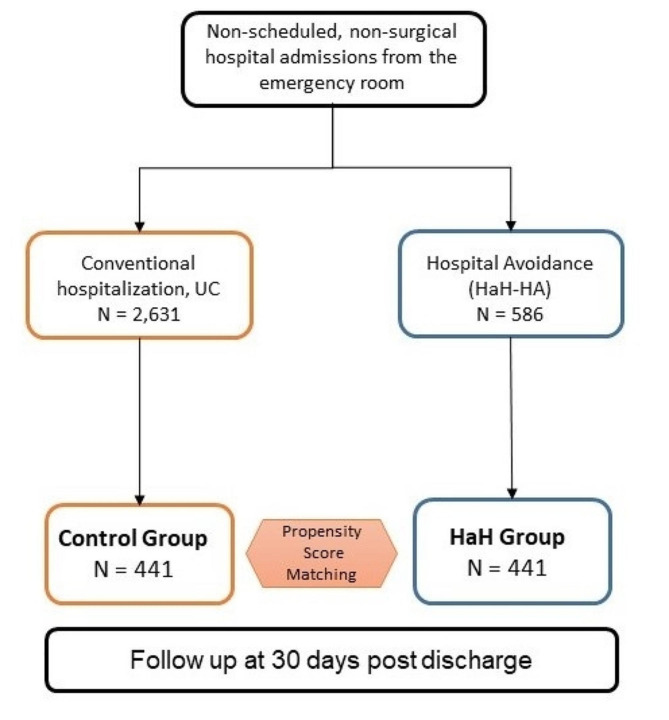
Methods: A retrospective cost-consequence analysis of all first episodes of HaH-HA, directly admitted from the emergency room (ER) in 2017-2018, was carried out with a health system perspective. HaH-HA was compared with a propensity-score-matched group of contemporary patients admitted to conventional hospitalization (Controls). Mortality, re-admissions, ER visits, and direct healthcare costs were evaluated.
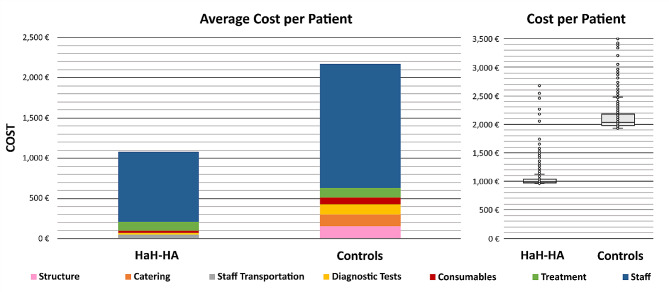
Results: HaH-HA and Controls (n = 441 each) were comparable in terms of age (73 [SD16] vs. 74 [SD16]), gender (male, 57% vs. 59%), multimorbidity, healthcare expenditure during the previous year, case mix index of the acute episode, and main diagnosis at discharge. HaH-HA presented lower mortality during the episode (0 vs. 19 (4.3%); p < 0.001). At 30 days post-discharge, HaH-HA and Controls showed similar re-admission rates; however, ER visits were lower in HaH-HA than in Controls (28 (6.3%) vs. 34 (8.1%); p = 0.044). Average costs per patient during the episode were lower in the HaH-HA group (€ 1,078) than in Controls (€ 2,171). Likewise, healthcare costs within the 30 days post-discharge were also lower in HaH-Ha than in Controls (p < 0.001).
Conclusions: The study showed higher performance and cost reductions of HaH-HA in a real-world setting. The identification of sources of savings facilitates scaling of hospital avoidance.
Registration: ClinicalTrials.gov (26/04/2017; NCT03130283).
Keywords: Early readmissions; Health services research; Hospital at home; Implementation science; Transitional care.
© 2024. The Author(s).
Conflict of interest statement
All authors have disclosed no conflicts of interest.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
