

Comparison of the Effects of Lidocaine and Amiodarone on Patients With Cardiac Arrest: A Systematic Review and Meta-Analysis
- PMID: 38623114
- PMCID: PMC11017951
- DOI: 10.7759/cureus.56037
Comparison of the Effects of Lidocaine and Amiodarone on Patients With Cardiac Arrest: A Systematic Review and Meta-Analysis
Abstract
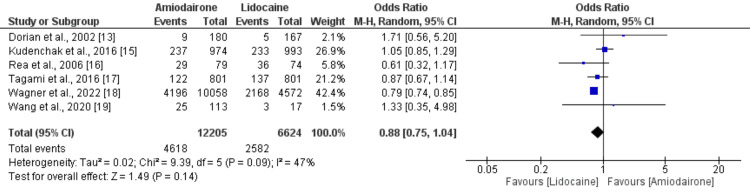
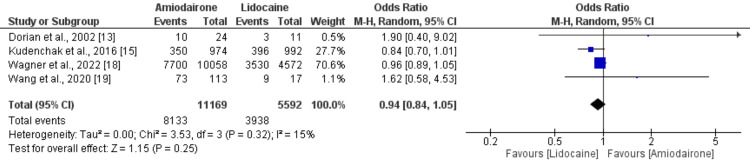
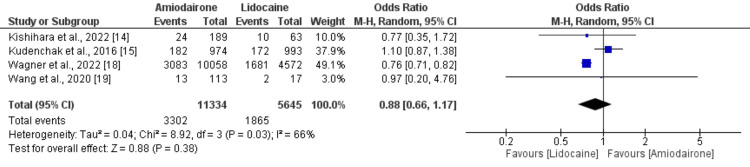
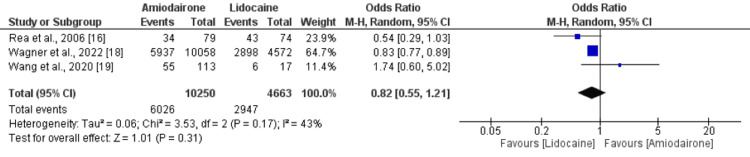
The objective of this study was to compare the impact of amiodarone and lidocaine on survival and neurological outcomes following cardiac arrest. A systematic review of randomized controlled trials (RCTs) as well as cohort and cross-sectional trials was undertaken, adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Potential relevant studies were searched in databases, including PubMed, Embase, Cochrane Library, and Web of Science, from the beginning of databases to February 15, 2024. Outcomes assessed in this study were survival to hospital discharge, survival to hospital admission or 24 hours, favorable neurological outcomes, and return of spontaneous circulation (ROSC). A total of seven studies (five observational and two RCTs) were included in this meta-analysis encompassing 19,081 patients with cardiac arrest. Pooled analysis showed no difference between amiodarone and lidocaine in terms of survival to hospital discharge (odds ratio (OR): 0.88, 95% confidence interval (CI): 0.75 to 1.04), ROSC (OR: 0.94, 95% CI: 0.84 to 1.05, p-value: 0.25), favorable neurological outcomes (OR: 0.88, 95% CI: 0.66 to 1.17, p-value: 0.38), and survival to 24 hours (OR: 0.82, 95% CI: 0.55 to 1.21, p-value: 0.31). While lidocaine demonstrated a slight survival advantage, the differences were statistically insignificant. Similarly, no significant variations were observed in ROSC incidence, neurological outcomes, or survival at 24 hours. These findings align with current guidelines but underscore the necessity for further rigorous RCTs to provide conclusive recommendations.
Keywords: amiodarone; cardiac arrest; lidocaine; meta-analysis; mortality.
Copyright © 2024, Sinha et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of amiodarone and lidocaine on shock-refractory cardiac arrest: a systematic review and meta-analysis.Kardiol Pol. 2020 Oct 23;78(10):999-1007. doi: 10.33963/KP.15483. Epub 2020 Jul 6. Kardiol Pol. 2020. PMID: 32627999
-
Comparison the efficacy of amiodarone and lidocaine for cardiac arrest: A network meta-analysis.Medicine (Baltimore). 2023 Apr 14;102(15):e33195. doi: 10.1097/MD.0000000000033195. Medicine (Baltimore). 2023. PMID: 37058064 Free PMC article.
-
Comparative Effectiveness of Amiodarone and Lidocaine for the Treatment of In-Hospital Cardiac Arrest.Chest. 2023 May;163(5):1109-1119. doi: 10.1016/j.chest.2022.10.024. Epub 2022 Nov 2. Chest. 2023. PMID: 36332663
-
Outcomes associated with amiodarone and lidocaine in the treatment of in-hospital pediatric cardiac arrest with pulseless ventricular tachycardia or ventricular fibrillation.Resuscitation. 2014 Mar;85(3):381-6. doi: 10.1016/j.resuscitation.2013.12.008. Epub 2013 Dec 19. Resuscitation. 2014. PMID: 24361455 Free PMC article.
-
Effectiveness of antiarrhythmic drugs for shockable cardiac arrest: A systematic review.Resuscitation. 2018 Nov;132:63-72. doi: 10.1016/j.resuscitation.2018.08.025. Epub 2018 Sep 1. Resuscitation. 2018. PMID: 30179691
References
-
- Outcomes of in-hospital cardiac arrest: a review of the evidence. DiLibero J, Misto K. Crit Care Nurs Clin North Am. 2021;33:343–356. - PubMed
-
- The role of inflammatory cytokines in cardiac arrest. Jou C, Shah R, Figueroa A, Patel JK. J Intensive Care Med. 2020;35:219–224. - PubMed
-
- The immunology of the post-cardiac arrest syndrome. Cunningham CA, Coppler PJ, Skolnik AB. Resuscitation. 2022;179:116–123. - PubMed
-
- Cardiac arrest caused by anaphylaxis refractory to prompt management. Park H, Kim SM, Kim WY. Am J Emerg Med. 2022;61:74–80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources