

doi: 10.1097/CLD.0000000000000135.
eCollection 2024 Jan-Jun.
Neonatal cholestasis: Timely triumph
Affiliations
- PMID: 38623148
- PMCID: PMC11018145
- DOI: 10.1097/CLD.0000000000000135
Item in Clipboard
Neonatal cholestasis: Timely triumph
Clin Liver Dis (Hoboken).
.
No abstract available
Conflict of interest statement
Jennifer Vittorio consults for and advises Mirum Pharma. The remaining authors have no conflicts to report
Figures

Percutaneous transhepatic cholecysto-cholangiography (PTCC). [A] Image demonstrates contrast filling the GB and common bile duct (black arrow) with reflux into the PD and free passage into the duodenum (D). Upstream, there is a beaded and truncated appearance of the common hepatic duct (white arrow) without contrast opacification of the intrahepatic bile ducts despite provocative maneuvers. Findings suggest biliary atresia. [B] PTCC is performed in a 1-month-old with normal biliary tree morphology. The needle resides within a normal contrast-opacified GB. A normal common bile duct (black arrow) is shown. Iodinated contrast media flows freely into the duodenum (D). Upstream, there is a normal division of the right and left intrahepatic ducts (white arrows). Abbreviations: D, duodenum; GB, gallbladder; PD, pancreatic duct; PTCC, Percutaneous transhepatic cholecysto-cholangiography.
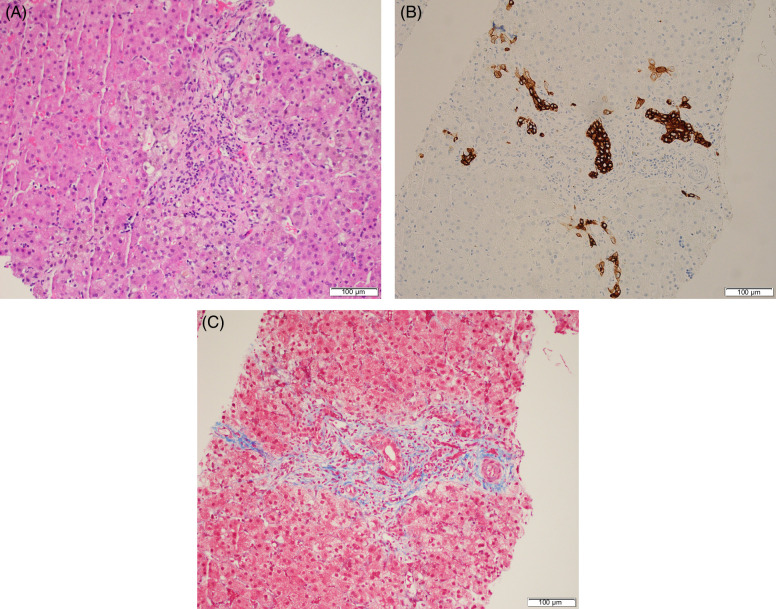
Percutaneous liver biopsy demonstrates bile duct injury with portal edema, fibrous expansion of the portal tracts, and prominent ductular reaction (A). Bile duct proliferation is further highlighted by cytokeratin 7 immunohistochemistry (B). Trichrome stain demonstrates focal septal formation (C).
References
-
- Fawaz R, Baumann U, Ekong U, Fischler B, Hadzic N, Mack CL, et al. . Guideline for the Evaluation of Cholestatic Jaundice in Infants: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2017;64:154–168. - PubMed
-
- Harpavat S, Ramraj R, Finegold MJ, Brandt ML, Hertel PM, Fallon SC, et al. . Newborn direct or conjugated bilirubin measurements as a potential screen for biliary atresia. J Pediatr Gastroenterol Nutr. 2016;62:799–803. - PubMed
-
- Heinz N, Vittorio J. Treatment of cholestasis in infants and young children. Curr Gastroenterol Rep. 2023;25:344–354. - PubMed
-
- Davenport M, Kronfli R, Makin E. Advances in understanding of biliary atresia pathogenesis and progression - A riddle wrapped in a mystery inside an enigma. Expert Rev Gastroenterol Hepatol. 2023;17:343–352. - PubMed
LinkOut - more resources
Full Text Sources
