

Faster Bone Gap Union in Medial Opening Wedge High Tibial Osteotomy With 3D-Printed Synthetic Bioresorbable Polycaprolactone and Tricalcium Phosphate Osteotomy Gap Fillers Compared to Allogeneic Osteotomy Gap Fillers: A Retrospective Matched-Pair Cohort Study
- PMID: 38624072
- PMCID: PMC11569676
- DOI: 10.1177/19476035241246609
Faster Bone Gap Union in Medial Opening Wedge High Tibial Osteotomy With 3D-Printed Synthetic Bioresorbable Polycaprolactone and Tricalcium Phosphate Osteotomy Gap Fillers Compared to Allogeneic Osteotomy Gap Fillers: A Retrospective Matched-Pair Cohort Study
Abstract
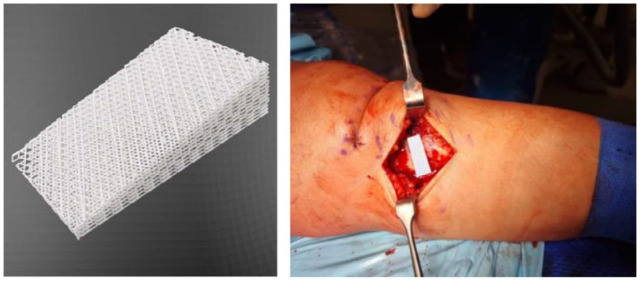
Objective: The use of synthetic bone substitute material (BSM) as osteotomy gap fillers have been reported to improve outcomes in medial opening wedge high tibial osteotomy (MOWHTO). This study aims to evaluate the early radiological outcomes (bone union) and complication rates of the novel patient-specific 3D-printed honeycomb-structured polycaprolactone and tricalcium phosphate (PCL-TCP) synthetic graft compared to allogeneic bone grafts as an osteotomy gap filler in MOWHTO.
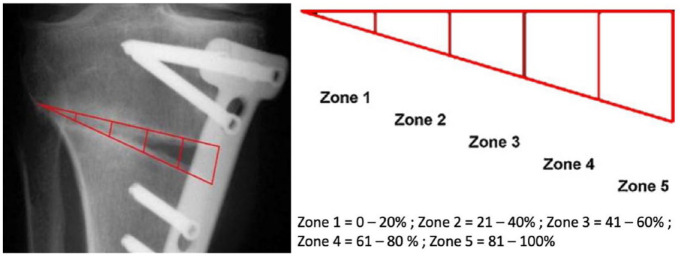
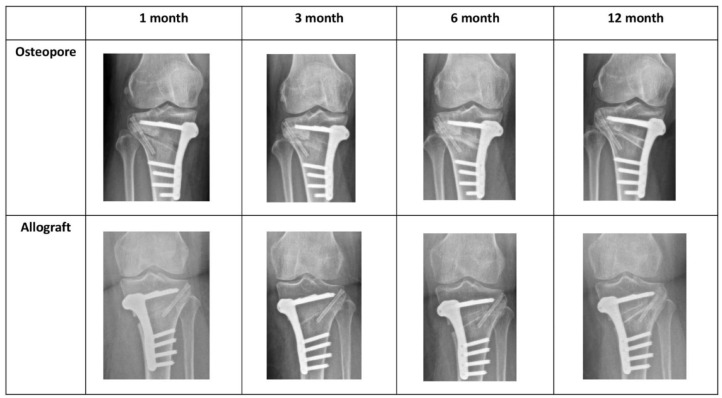
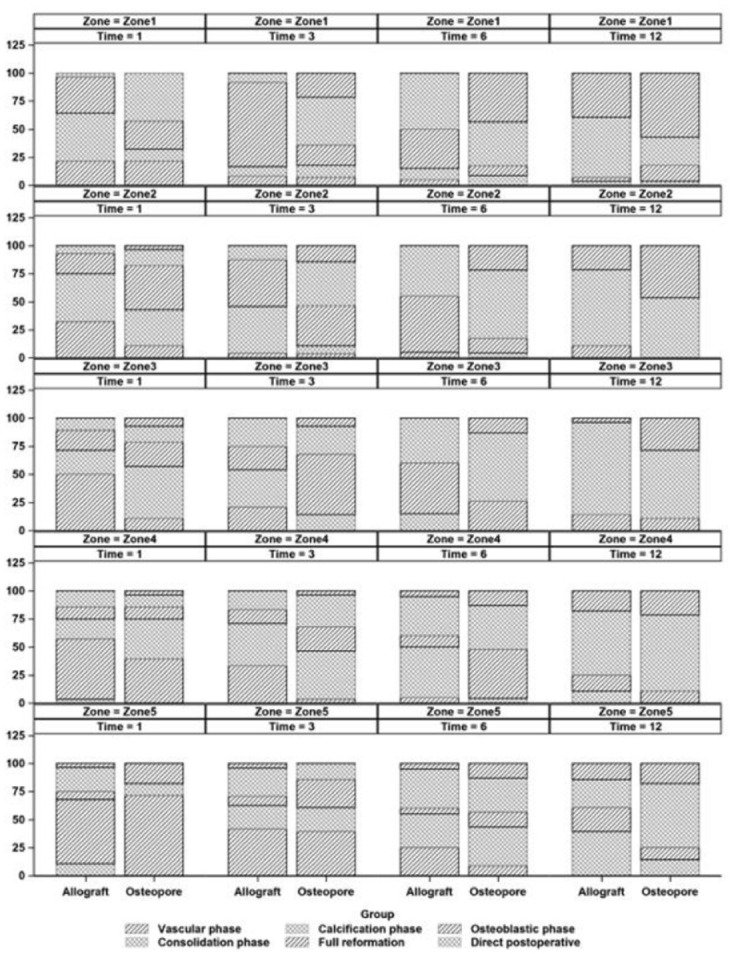
Methods: A retrospective matched-pair analysis of patients who underwent MOWHTO with either PCL-TCP synthetic graft or allogenic femoral head allograft as osteotomy gap filler was performed. The osteotomy gap was split into equal zones (Zone 1-5), and bone union was evaluated on anteroposterior radiographs based on the van Hemert classification at 1, 3, 6, and 12 months postoperatively. Postoperative complications including infection, lateral hinge fractures, and persistent pain was measured. The study and control group were matched for age, smoking status, diabetes mellitus, and osteotomy gap size.
Results: Significantly greater bone union progression was observed in the PCL-TCP group than in the allograft group at 1 month (Zones 1-3), 3 months (Zones 1-4), 6 months (Zones 1-2, 4), and 12 months (Zones 2-3, 5) postoperatively (P < 0.05). No significant difference in complications rates was noted between the two groups at 1 year.
Conclusions: Bone union rates observed in patients who underwent MOWHTO with the PCL-TCP synthetic graft osteotomy gap filler were superior to those in the allograft group at 1 year postoperatively, with no significant difference in complication rates (postoperative infection, lateral hinge fractures, and persistent pain).
Keywords: 3D-printing; allograft; bone union; medial opening wedge high tibial; osteotomy; polycaprolactone and tricalcium phosphate.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Zuiderbaan HA, van der List JP, Kleeblad LJ, Appelboom P, Kort NP, Pearle AD, et al. Modern indications, results, and global trends in the use of unicompartmental knee arthroplasty and high tibial osteotomy in the treatment of isolated medial compartment osteoarthritis. Am J Orthop (Belle Mead NJ). 2016;45(6):E355-61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
