

Bowel preparation for elective colorectal resection: multi-treatment machine learning analysis on 6241 cases from a prospective Italian cohort
- PMID: 38625550
- PMCID: PMC11021318
- DOI: 10.1007/s00384-024-04627-6
Bowel preparation for elective colorectal resection: multi-treatment machine learning analysis on 6241 cases from a prospective Italian cohort
Abstract
Background: Current evidence concerning bowel preparation before elective colorectal surgery is still controversial. This study aimed to compare the incidence of anastomotic leakage (AL), surgical site infections (SSIs), and overall morbidity (any adverse event, OM) after elective colorectal surgery using four different types of bowel preparation.
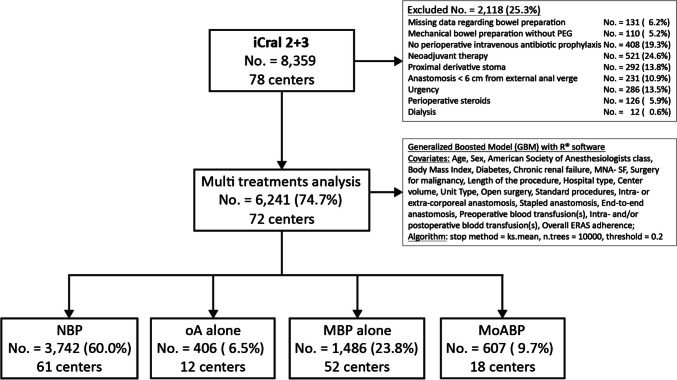
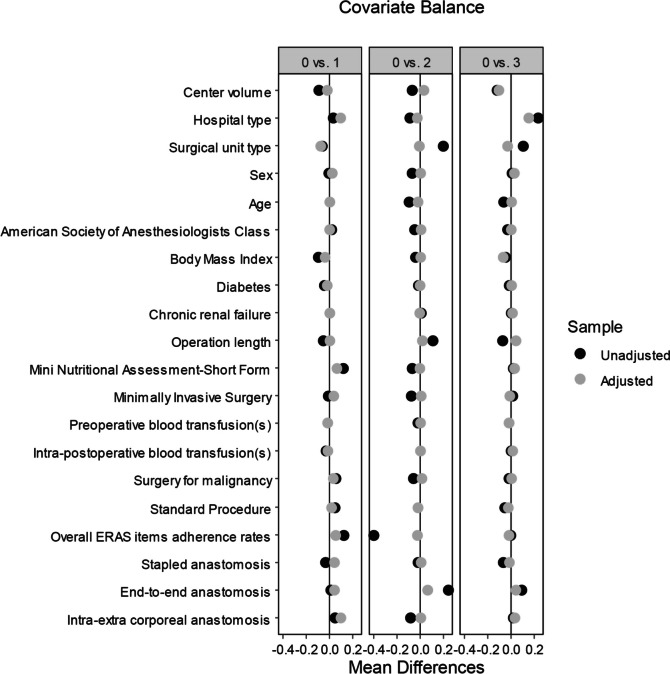
Methods: A prospective database gathered among 78 Italian surgical centers in two prospective studies, including 6241 patients who underwent elective colorectal resection with anastomosis for malignant or benign disease, was re-analyzed through a multi-treatment machine-learning model considering no bowel preparation (NBP; No. = 3742; 60.0%) as the reference treatment arm, compared to oral antibiotics alone (oA; No. = 406; 6.5%), mechanical bowel preparation alone (MBP; No. = 1486; 23.8%), or in combination with oAB (MoABP; No. = 607; 9.7%). Twenty covariates related to biometric data, surgical procedures, perioperative management, and hospital/center data potentially affecting outcomes were included and balanced into the model. The primary endpoints were AL, SSIs, and OM. All the results were reported as odds ratio (OR) with 95% confidence intervals (95% CI).
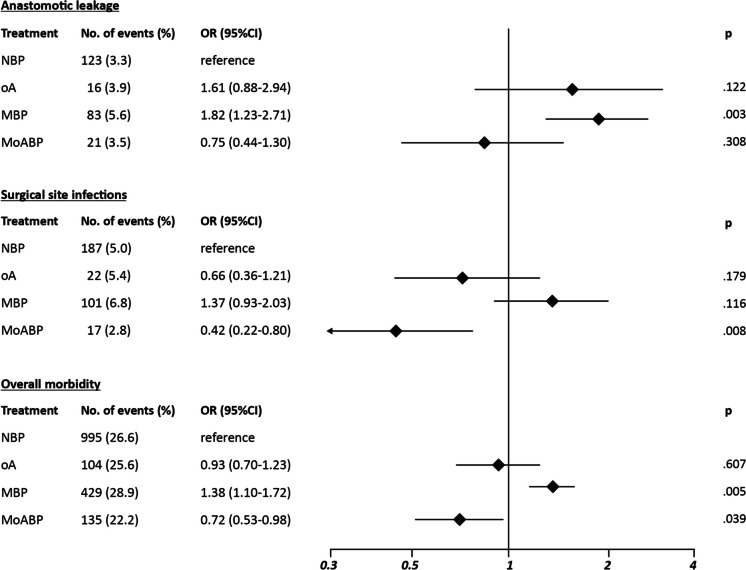
Results: Compared to NBP, MBP showed significantly higher AL risk (OR 1.82; 95% CI 1.23-2.71; p = .003) and OM risk (OR 1.38; 95% CI 1.10-1.72; p = .005), no significant differences for all the endpoints were recorded in the oA group, whereas MoABP showed a significantly reduced SSI risk (OR 0.45; 95% CI 0.25-0.79; p = .008).
Conclusions: MoABP significantly reduced the SSI risk after elective colorectal surgery, therefore representing a valid alternative to NBP.
Keywords: Anastomotic leakage; Colorectal surgery; Mechanical bowel preparation; Oral antibiotics; Surgical site infections.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Miettinen RP, Laitinen ST, Mäkelä JT, Pääkkönen ME (2000) Bowel preparation with oral polyethylene glycol electrolyte solution vs. no preparation in elective open colorectal surgery: prospective, randomized study. Dis Colon Rectum 43:669–675 - PubMed
-
- Bucher P, Gervaz P, Soravia C, Mermillod B, Erne M, Morel P (2005) Randomized clinical trial of mechanical bowel preparation versus no preparation before elective left-sided colorectal surgery. Br J Surg 92:409–414 - PubMed
-
- Catarci M, Guadagni S, Masedu F et al (2024) Mechanical bowel preparation in elective colorectal surgery: a propensity score-matched analysis of the Italian colorectal anastomotic leakage (iCral) study group prospective cohorts. Updates Surg 76(1):107–117 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
