

Glucose Control and Risk of Symptomatic Intracerebral Hemorrhage Following Thrombolysis for Acute Ischemic Stroke: A SHINE Trial Analysis
- PMID: 38626363
- PMCID: PMC11175634
- DOI: 10.1212/WNL.0000000000209323
Glucose Control and Risk of Symptomatic Intracerebral Hemorrhage Following Thrombolysis for Acute Ischemic Stroke: A SHINE Trial Analysis
Abstract
Background and objectives: Baseline hyperglycemia is associated with worse outcomes in acute ischemic stroke (AIS), including higher risk of symptomatic intracerebral hemorrhage (sICH) following treatment with thrombolysis. Prospective data are lacking to inform management of post-thrombolysis hyperglycemia. In a prespecified analysis from the Stroke Hyperglycemia Insulin Network Effort (SHINE) trial of hyperglycemic stroke management, we hypothesized that post-thrombolysis hyperglycemia is associated with a higher risk of sICH.
Methods: Hyperglycemic AIS patients <12 hours onset were randomized to intensive insulin (target range 80-130 mg/dL) vs standard sliding scale (80-179 mg/dL) over a 72-hour period, stratified by treatment with thrombolysis. Three board-certified vascular neurologists independently reviewed all sICH events occurring within 7 days, defined by neurologic deterioration of ≥4 points on the NIH Stroke Scale (NIHSS). Associations between blood glucose control and sICH were analyzed using logistic regression accounting for NIHSS, age, systolic blood pressure, onset to thrombolysis time, and endovascular therapy (odds ratios [OR], 95% CI). Additional analysis compared patients in a high-risk group (age older than 60 years and NIHSS ≥8) vs all others. Categorical variables and outcomes were compared using the χ2 test (p < 0.05).
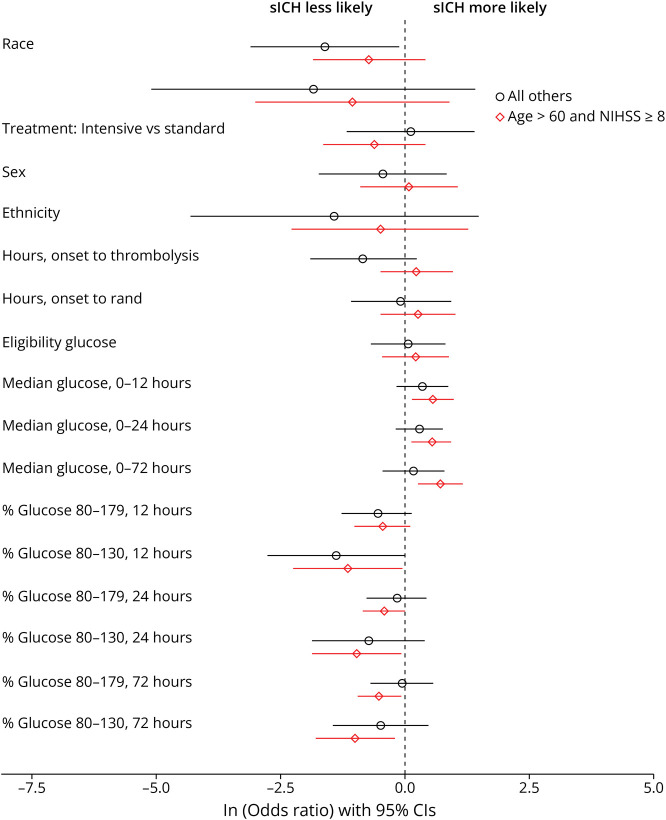
Results: Of 1151 SHINE participants, 725 (63%) received thrombolysis (median age 65 years, 46% women, 29% Black, 18% Hispanic). The median NIHSS was 7, baseline blood glucose was 187 (interquartile range 153-247) mg/dL, and 80% were diabetic. Onset to thrombolysis time was 2.2 hours (1.6-2.9). Post-thrombolysis sICH occurred in 3.6% (3.0% intensive vs 4.3% standard glucose control, OR 1.10, 0.60-2.01, p = 0.697). In the first 12 hours, every 10 mg/dL higher glucose increased the odds of sICH (OR 1.08, 1.03-1.14, p = 0.004), and a greater proportion of glucose measures in the normal range (80-130 mg/dL) decreased the odds of sICH (0.89, 0.80-0.99, p = 0.030). These associations were strongest in the high-risk group (age older than 60 years and NIHSS ≥8).
Discussion: In this prespecified analysis from the SHINE trial, intensive insulin therapy was not associated with a reduced risk of post-thrombolysis sICH compared with standard sliding scale. However, early post-thrombolysis hyperglycemia was associated with a higher risk of sICH overall, particularly in older patients with more severe strokes. Further prospective research is warranted to address the risk of sICH in hyperglycemic stroke patients undergoing endovascular therapy.
Trial registration information: NCT01369069.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical