

Neoantigen-targeted dendritic cell vaccination in lung cancer patients induces long-lived T cells exhibiting the full differentiation spectrum
- PMID: 38626769
- PMCID: PMC11148567
- DOI: 10.1016/j.xcrm.2024.101516
Neoantigen-targeted dendritic cell vaccination in lung cancer patients induces long-lived T cells exhibiting the full differentiation spectrum
Abstract
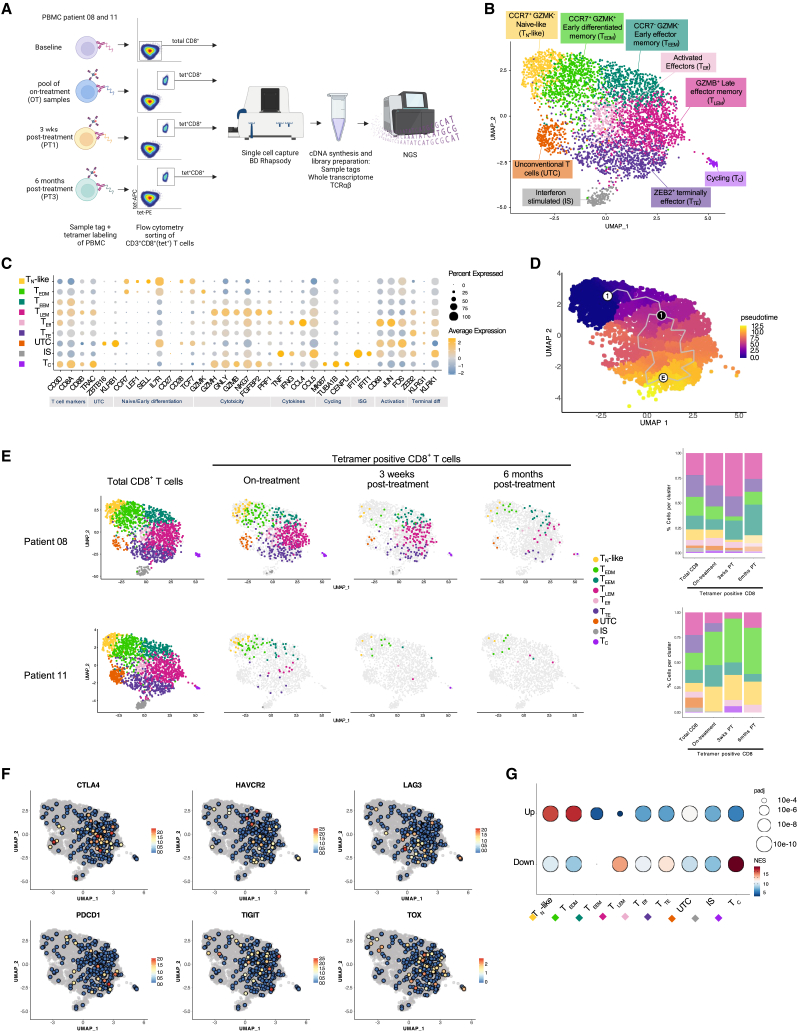
Non-small cell lung cancer (NSCLC) is known for high relapse rates despite resection in early stages. Here, we present the results of a phase I clinical trial in which a dendritic cell (DC) vaccine targeting patient-individual neoantigens is evaluated in patients with resected NSCLC. Vaccine manufacturing is feasible in six of 10 enrolled patients. Toxicity is limited to grade 1-2 adverse events. Systemic T cell responses are observed in five out of six vaccinated patients, with T cell responses remaining detectable up to 19 months post vaccination. Single-cell analysis indicates that the responsive T cell population is polyclonal and exhibits the near-entire spectrum of T cell differentiation states, including a naive-like state, but excluding exhausted cell states. Three of six vaccinated patients experience disease recurrence during the follow-up period of 2 years. Collectively, these data support the feasibility, safety, and immunogenicity of this treatment in resected NSCLC.
Keywords: T cell responses; cell therapy; clinical trial; dendritic cell vaccine; immunotherapy; neoantigens; non-small cell lung cancer; personalized vaccine.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
