

The Pancreatic Cancer Early Detection (PRECEDE) Study is a Global Effort to Drive Early Detection: Baseline Imaging Findings in High-Risk Individuals
- PMID: 38626807
- PMCID: PMC12344727
- DOI: 10.6004/jnccn.2023.7097
The Pancreatic Cancer Early Detection (PRECEDE) Study is a Global Effort to Drive Early Detection: Baseline Imaging Findings in High-Risk Individuals
Abstract
Background: Pancreatic adenocarcinoma (PC) is a highly lethal malignancy with a survival rate of only 12%. Surveillance is recommended for high-risk individuals (HRIs), but it is not widely adopted. To address this unmet clinical need and drive early diagnosis research, we established the Pancreatic Cancer Early Detection (PRECEDE) Consortium.
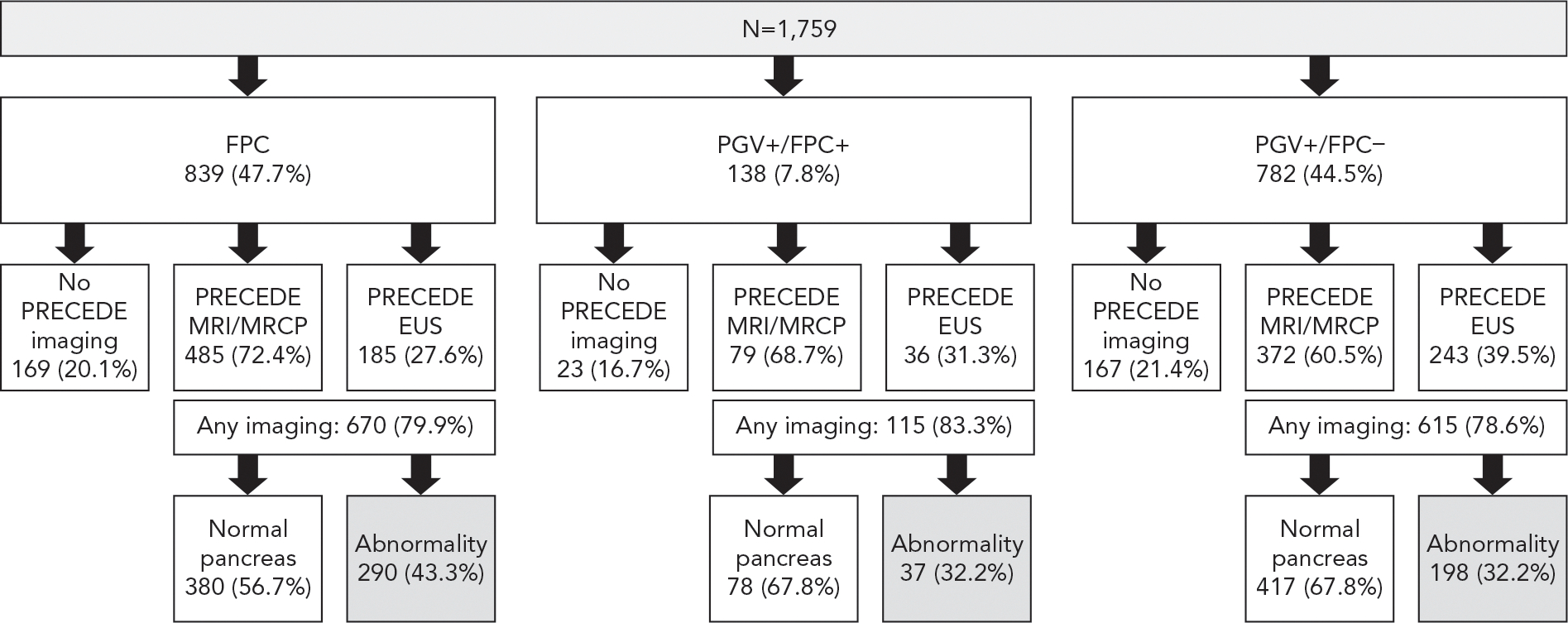
Methods: PRECEDE is a multi-institutional international collaboration that has undertaken an observational prospective cohort study. Individuals (aged 18-90 years) are enrolled into 1 of 7 cohorts based on family history and pathogenic germline variant (PGV) status. From April 1, 2020, to November 21, 2022, a total of 3,402 participants were enrolled in 1 of 7 study cohorts, with 1,759 (51.7%) meeting criteria for the highest-risk cohort (Cohort 1). Cohort 1 HRIs underwent germline testing and pancreas imaging by MRI/MR-cholangiopancreatography or endoscopic ultrasound.
Results: A total of 1,400 participants in Cohort 1 (79.6%) had completed baseline imaging and were subclassified into 3 groups based on familial PC (FPC; n=670), a PGV and FPC (PGV+/FPC+; n=115), and a PGV with a pedigree that does not meet FPC criteria (PGV+/FPC-; n=615). One HRI was diagnosed with stage IIB PC on study entry, and 35.1% of HRIs harbored pancreatic cysts. Increasing age (odds ratio, 1.05; P<.001) and FPC group assignment (odds ratio, 1.57; P<.001; relative to PGV+/FPC-) were independent predictors of harboring a pancreatic cyst.
Conclusions: PRECEDE provides infrastructure support to increase access to clinical surveillance for HRIs worldwide, while aiming to drive early PC detection advancements through longitudinal standardized clinical data, imaging, and biospecimen captures. Increased cyst prevalence in HRIs with FPC suggests that FPC may infer distinct biological processes. To enable the development of PC surveillance approaches better tailored to risk category, we recommend adoption of subclassification of HRIs into FPC, PGV+/FPC+, and PGV+/FPC- risk groups by surveillance protocols.
Trial registration: ClinicalTrials.gov NCT04970056.
Figures



References
-
- Yu J, Yang X, He W, et al. Burden of pancreatic cancer along with attributable risk factors in Europe between 1990 and 2019, and projections until 2039. Int J Cancer 2021;149:993–1001. - PubMed
-
- Pourshams A, Sepanlou SG, Ikuta KS, et al. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol 2019;4:934–947. - PMC - PubMed
-
- Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin 2023;73:17–48. - PubMed
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014;371:1039–1049. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
