

Accuracy of MRI-ultrasound fusion-guided and systematic biopsy of the prostate
- PMID: 38627253
- PMCID: PMC11135791
- DOI: 10.1093/bjr/tqae080
Accuracy of MRI-ultrasound fusion-guided and systematic biopsy of the prostate
Abstract
Objectives: Prostate multiparametric MRI (mpMRI) with subsequent targeted biopsy of suspicious lesions has a critical role in the diagnostic workup of prostate cancer. The objective was to evaluate the diagnostic accuracy of systematic biopsies, targeted biopsies, and the combination of both in prostate cancer detection.
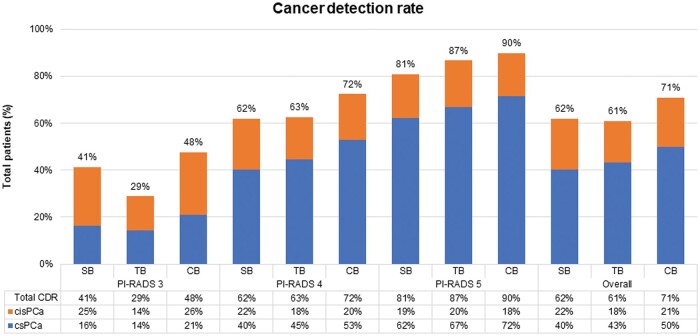
Methods: From January 1, 2013 to June 1, 2022, biopsy-naïve and prior biopsy-negative patients who underwent both systematic and targeted biopsies were included. MRIs were evaluated according to PI-RADS with biopsy threshold set at PI-RADS ≥3. Systematic biopsies consisted of 8-12 cores, based on prostate volume. Overall prostate cancer and clinically significant cancer (Gleason Score ≥3 + 4) detection rates were stratified based on PI-RADS and location within the prostate, and compared between biopsy types using McNemar test.
Results: Among 867 patients, 615 had prostate cancer, with 434 clinically significant cases. Overall detection rates were: PI-RADS 3 48%, PI-RADS 4 72%, and PI-RADS 5 90%. Detection rates for clinically significant cancer were 21%, 53%, and 72%, respectively. The combination of biopsy methods was most accurate in detecting clinically significant prostate cancer (P < .001). Targeted biopsies alone detected more clinically significant prostate cancer than systematic biopsies alone (43.1% vs 40.3%, P = .046). For posterior PI-RADS 5 lesions, no statistically significant difference was found between all biopsy methods.
Conclusions: In the detection of clinically significant prostate cancer, the combination of systematic and targeted biopsies proves most effective. Targeted biopsies rarely missed significant cancer for posterior PI-RADS 5 lesions, suggesting systematic biopsies could be reserved for instances where targeted biopsy results are negative.
Advances in knowledge: This study emphasizes on the efficacy of mpMRI and targeted biopsies in suspected prostate cancer in real-world clinical context. For PI-RADS 5 lesions, systematic biopsies provide limited clinical benefit and may only be necessary when targeted biopsy results are negative.
Keywords: MRI-ultrasound fusion biopsy; PI-RADS; biopsy-naïve; prior biopsy negative; prostate cancer; systematic biopsy; targeted biopsy.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
-
- Kasivisvanathan V, Stabile A, Neves JB, et al. Magnetic resonance imaging-targeted biopsy versus systematic biopsy in the detection of prostate cancer: a systematic review and meta-analysis. Eur Urol. 2019;76(3):284-303. - PubMed
-
- Schoots IG, Roobol MJ, Nieboer D, Bangma CH, Steyerberg EW, Hunink MG. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: a systematic review and meta-analysis. Eur Urol. 2015;68(3):438-450. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
