

Bright light therapy versus physical exercise to prevent co-occurring depression in adolescents and young adults with attention-deficit/hyperactivity disorder: a multicentre, three-arm, randomised controlled, pilot phase-IIa trial
- PMID: 38627266
- PMCID: PMC11946981
- DOI: 10.1007/s00406-024-01784-1
Bright light therapy versus physical exercise to prevent co-occurring depression in adolescents and young adults with attention-deficit/hyperactivity disorder: a multicentre, three-arm, randomised controlled, pilot phase-IIa trial
Abstract
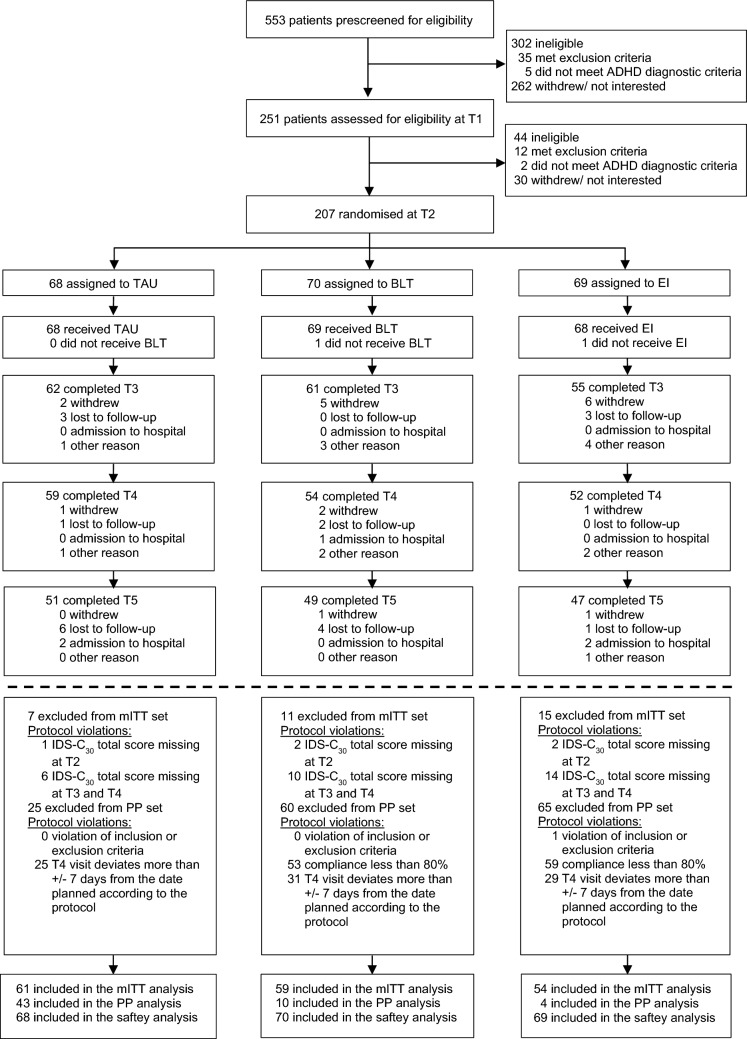
Depression is common in attention-deficit/hyperactivity disorder (ADHD), but preventive behavioural interventions are lacking. This randomised controlled, pilot phase-IIa trial aimed to study a physical exercise intervention (EI) and bright light therapy (BLT)-both implemented and monitored in an individual, naturalistic setting via a mobile health (m-health) system-for feasibility of trial design and interventions, and to estimate their effects on depressive symptoms in young people with ADHD. Two hundred seven participants aged 14-45 years were randomised to 10-week add-on intervention of either BLT (10,000 lx; daily 30-min sessions) (n = 70), EI (aerobic and muscle-strengthening activities 3 days/ week) (n = 69), or treatment-as-usual (TAU) (n = 68), of whom 165 (80%) were retained (BLT: n = 54; EI: n = 52; TAU: n = 59). Intervention adherence (i.e. ≥ 80% completed sessions) was very low for both BLT (n = 13, 22%) and EI (n = 4, 7%). Usability of the m-health system to conduct interventions was limited as indicated by objective and subjective data. Safety was high and comparable between groups. Changes in depressive symptoms (assessed via observer-blind ratings, Inventory of Depressive Symptomatology) between baseline and end of intervention were small (BLT: -0.124 [95% CI: -2.219, 1.971], EI: -2.646 [95% CI: -4.777, -0.515], TAU: -1.428 [95% CI: -3.381, 0.526]) with no group differences [F(2,153) = 1.45, p = 0.2384]. These findings suggest that the m-health approach did not achieve feasibility of EI and BLT in young people with ADHD. Prior to designing efficacy studies, strategies how to achieve high intervention adherence should be specifically investigated in this patient group. TRIAL REGISTRATION: ClinicalTrials.gov, NCT03371810, 13 December 2017.
Keywords: Attention-deficit/hyperactivity disorder; Bright light therapy; Depression; Obesity; Physical exercise; Randomised controlled trial; m-Health.
© 2024. The Author(s).
Figures

References
-
- Franke B, Michelini G, Asherson P, Banaschewski T, Bilbow A, Buitelaar JK, Cormand B, Faraone SV, Ginsberg Y, Haavik J, Kuntsi J, Larsson H, Lesch K-P, Ramos-Quiroga JA, Réthelyi JM, Ribases M, Reif A (2018) Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. Eur Neuropsychopharmacol 28(10):1059–1088. 10.1016/j.euroneuro.2018.08.001 - PMC - PubMed
-
- Kittel-Schneider S, Arteaga-Henriquez G, Vasquez AA, Asherson P, Banaschewski T, Brikell I, Buitelaar J, Cormand B, Faraone SV, Freitag CM, Ginsberg Y, Haavik J, Hartman CA, Kuntsi J, Larsson H, Matura S, McNeill RV, Ramos-Quiroga JA, Ribases M, Romanos M, Vainieri I, Franke B, Reif A (2022) Non-mental diseases associated with ADHD across the lifespan: Fidgety Philipp and Pippi Longstocking at risk of multimorbidity? Neurosci Biobehav Rev 132:1157–1180. 10.1016/j.neubiorev.2021.10.035 - PubMed
-
- Libutzki B, Ludwig S, May M, Jacobsen RH, Reif A, Hartman CA (2019) Direct medical costs of ADHD and its comorbid conditions on basis of a claims data analysis. Eur Psychiatry 58:38–44. 10.1016/j.eurpsy.2019.01.019 - PubMed
-
- Biederman J, Ball SW, Monuteaux MC, Mick E, Spencer TJ, McCREARY M, Cote M, Faraone SV (2008) New insights into the comorbidity between ADHD and major depression in adolescent and young adult females. J Am Acad Child Adolesc Psychiatry 47(4):426–434. 10.1097/CHI.0b013e31816429d3 - PubMed
-
- Jacob CP, Romanos J, Dempfle A, Heine M, Windemuth-Kieselbach C, Kruse A, Reif A, Walitza S, Romanos M, Strobel A, Brocke B, Schäfer H, Schmidtke A, Böning J, Lesch K-P (2007) Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits and related disorders in a tertiary referral center. Eur Arch Psychiatry Clin Neurosci 257(6):309–317. 10.1007/s00406-007-0722-6 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
