

Temporal bone squamous cell carcinoma: Aggressive behavior coursing with cerebellar invasion and hydrocephalus
- PMID: 38628504
- PMCID: PMC11021098
- DOI: 10.25259/SNI_1017_2023
Temporal bone squamous cell carcinoma: Aggressive behavior coursing with cerebellar invasion and hydrocephalus
Abstract
Background: Temporal bone squamous cell carcinoma (TBSCC) is a very rare condition. The prognosis is dismal for advanced tumors. Due to its rarity, information in the literature is scarce. Here, we report a unique case of TBSCC with cerebellar invasion and hydrocephalus.
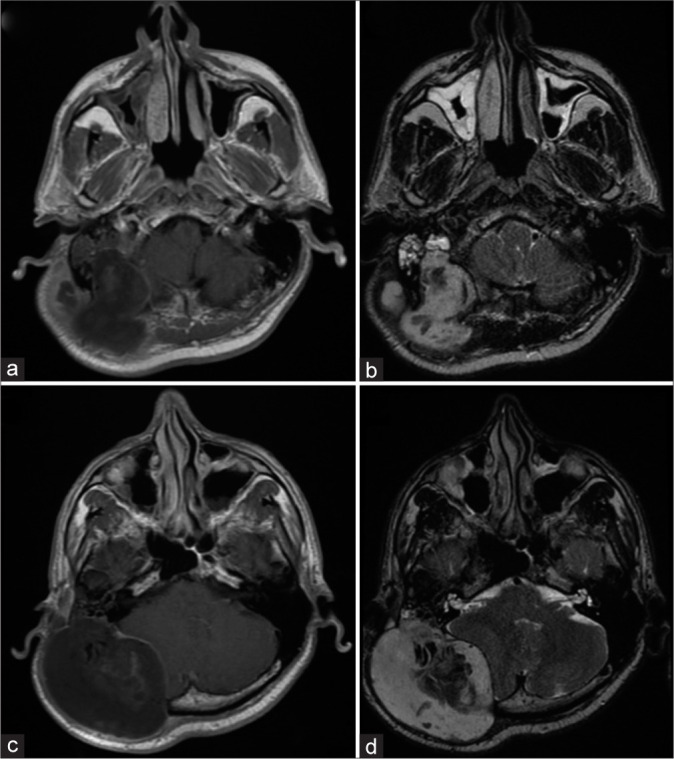
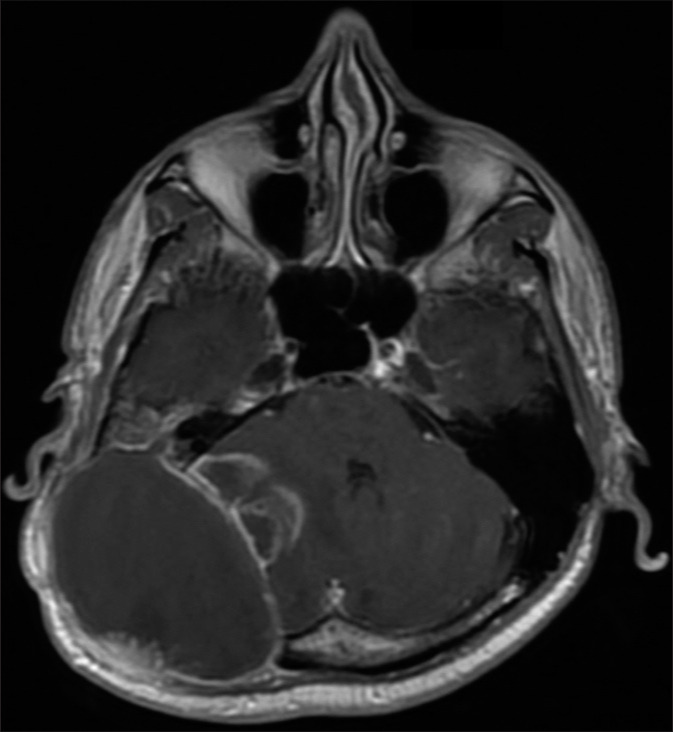
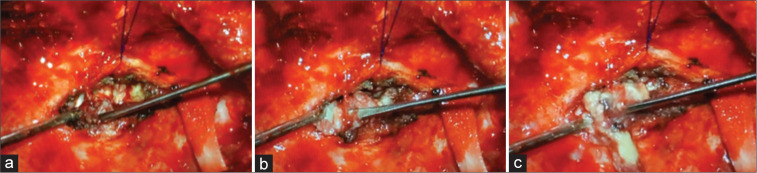
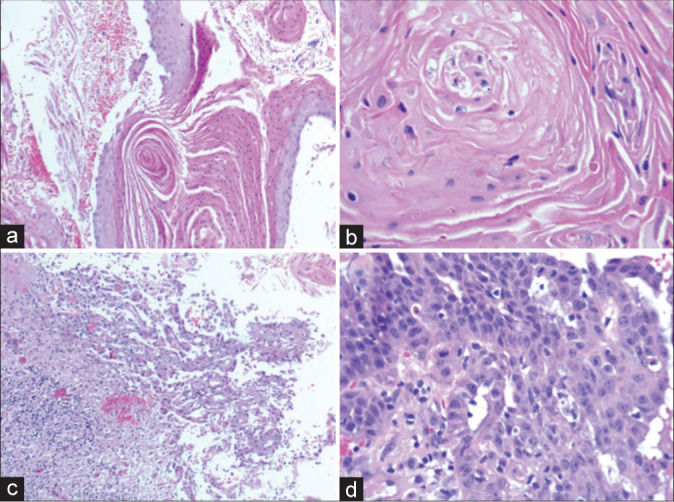
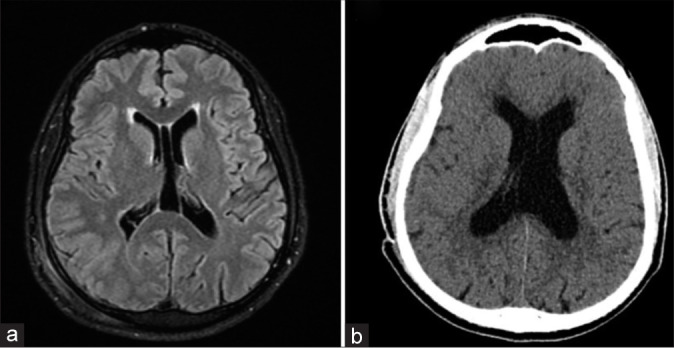
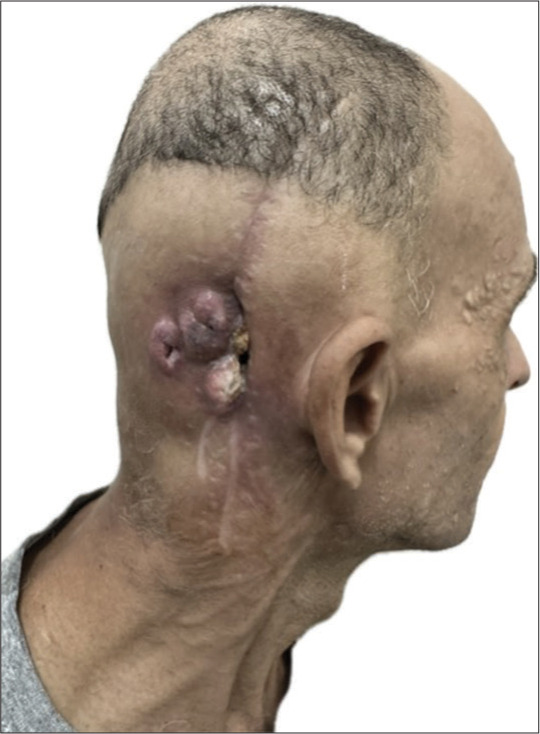
Case description: A 46-year-old reported right-sided hearing loss and a painful right retroauricular mass for 4 months. Magnetic resonance imaging revealed a 8.7 × 7.6 × 6.4 cm mass invading the right temporal and occipital bones. After a biopsy and 3 surgical procedures over 6 months, the diagnosis of TBSCC was obtained. Due to invasion of the cerebellar tissue and obstructive hydrocephalus, a ventriculoperitoneal shunt was performed. The patient was referred for adjuvant radiotherapy. However, palliative care was initiated due to tumor progression.
Conclusion: We report a case of advanced TBSCC with poor prognosis despite surgical treatment and radiotherapy. More data are necessary to provide new and better treatment to these patients.
Keywords: Cerebellum; Hydrocephalus; Squamous cell carcinoma; Temporal bone.
Copyright: © 2024 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Squamous cell carcinoma of the temporal bone: A current review.Laryngoscope Investig Otolaryngol. 2019 Nov 13;4(6):684-692. doi: 10.1002/lio2.330. eCollection 2019 Dec. Laryngoscope Investig Otolaryngol. 2019. PMID: 31890889 Free PMC article. Review.
-
Temporal Bone Squamous Cell Carcinoma: Molecular Markers Involved in Carcinogenesis, Behavior, and Prognosis: A Systematic Review.Int J Mol Sci. 2022 Apr 20;23(9):4536. doi: 10.3390/ijms23094536. Int J Mol Sci. 2022. PMID: 35562926 Free PMC article.
-
Long-term survival after immunotherapy for uncontrolled locally advanced temporal bone squamous cell carcinoma followed by chemoradiotherapy: A case report.Precis Radiat Oncol. 2024 Jun 28;8(2):99-105. doi: 10.1002/pro6.1233. eCollection 2024 Jun. Precis Radiat Oncol. 2024. PMID: 40336643 Free PMC article.
-
Tumor budding to investigate local invasion, metastasis and prognosis in temporal bone squamous cell carcinoma.Pathol Res Pract. 2022 Jan;229:153719. doi: 10.1016/j.prp.2021.153719. Epub 2021 Nov 28. Pathol Res Pract. 2022. PMID: 34953406
-
Temporal bone carcinoma: a first glance beyond the conventional clinical and pathological prognostic factors.Eur Arch Otorhinolaryngol. 2016 Oct;273(10):2903-10. doi: 10.1007/s00405-015-3811-6. Epub 2015 Oct 30. Eur Arch Otorhinolaryngol. 2016. PMID: 26518208 Review.
References
-
- Arena S, Keen M. Carcinoma of the middle ear and temporal bone. Am J Otol. 1998;9:351–6. - PubMed
-
- Arriaga M, Curtin H, Takahashi H, Hirsch BE, Kamerer DB. Staging proposal for external auditory meatus carcinoma based on preoperative clinical examination and computed tomography findings. Ann Otol Rhinol Laryngol. 1990;99:714–21. - PubMed
-
- Conley JJ. Cancer of the middle ear and temporal bone. N Y State J Med. 1974;74:1575–9. - PubMed
-
- Gidley PW, DeMonte F. Temporal bone malignancies. Neurosurg Clin N Am. 2013;24:97–110. - PubMed
Publication types
LinkOut - more resources
Full Text Sources