

Airway risk associated with patients in halo fixation
- PMID: 38628525
- PMCID: PMC11021081
- DOI: 10.25259/SNI_386_2023
Airway risk associated with patients in halo fixation
Abstract
Background: The halo fixation device introduces a significant obstacle for clinicians attempting to secure a definitive airway in trauma patients with cervical spine injuries. The authors sought to determine the airway-related mortality rate of adult trauma patients in halo fixation requiring endotracheal intubation.
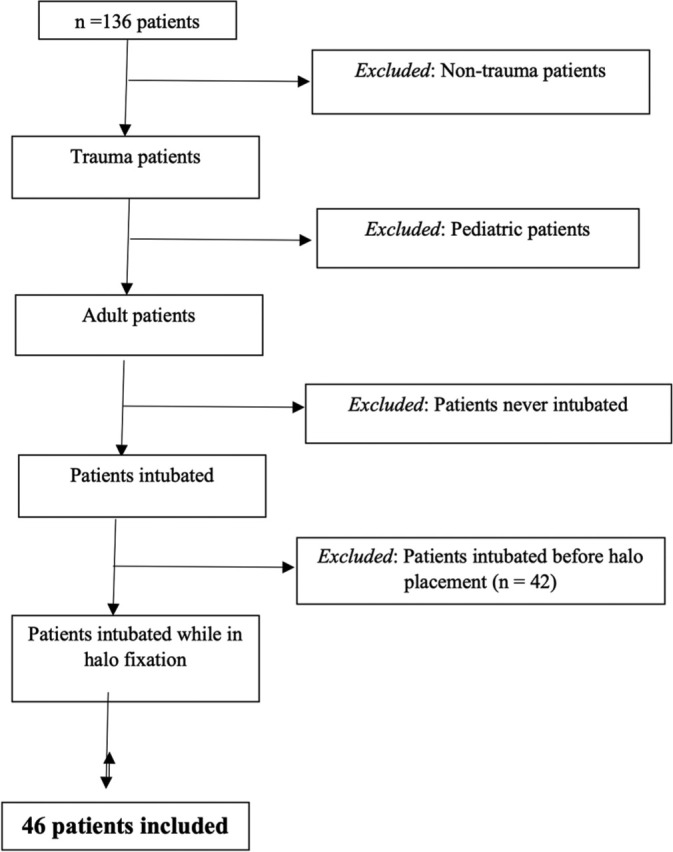
Methods: This study was a retrospective chart review of patients identified between 2007 and 2012. Only adult trauma patients who were intubated while in halo fixation were included in the study.
Results: A total of 46 patients underwent 60 intubations while in halo. On five occasions, (8.3%) patients were unable to be intubated and required an emergent surgical airway. Two (4.4%) of the patients out of our study population died specifically due to airway complications. Elective intubations had a failure rate of 5.8% but had no related permanent morbidity or mortality. In contrast to that, 25% of non-elective intubations failed and resulted in the deaths of two patients. The association between mortality and non-elective intubations was statistically highly significant (P = 0.0003).
Conclusion: The failed intubation and airway-related mortality rates of patients in halo fixation were substantial in this study. This finding suggests that the halo device itself may present a major obstacle in airway management. Therefore, heightened vigilance is appropriate for intubations of patients in halo fixation.
Keywords: Airway Management; Cervical Injury; Emergent Intubation; Halo Fixation; Loss of Airway Mortality; Tracheostomy; Trauma Intubation.
Copyright: © 2024 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
References
-
- Aprahamian C, Thompson BM, Finger WA, Darinz JC. Experimental cervical spine injury model: Evaluation of airway management and splinting techniques. Ann Emerg Med. 1984;13:584–7. - PubMed
-
- Avitsian R, Lin J, Lotto M, Ebrahim Z. Dexmedetomidine and awake fiberoptic intubation for possible cervical spine myelopathy: A clinical series. J Neurosurg Anesthesiol. 2005;17:97–9. - PubMed
-
- Bannister F, Macbeth R. Direct laryngoscopy and tracheal intubation. Lancet. 1944;2:651–4.
-
- Bellamy R, Pitt FW, Stauffer ES. Respiratory complications in traumatic quadriplegia: Analysis of 20 years’ experience. J Neurosurg. 1973;39:596–600. - PubMed
LinkOut - more resources
Full Text Sources