

Genomic Landscape and Clinical Features of Advanced Thyroid Carcinoma: A National Database Study in Japan
- PMID: 38630010
- PMCID: PMC11479701
- DOI: 10.1210/clinem/dgae271
Genomic Landscape and Clinical Features of Advanced Thyroid Carcinoma: A National Database Study in Japan
Abstract
Context: The relationship between the genomic profile and prognosis of advanced thyroid carcinoma requiring drug therapy has not been reported.
Objective: To evaluate the treatment period and overall survival time for each genetic alteration in advanced thyroid carcinoma that requires drug therapy.
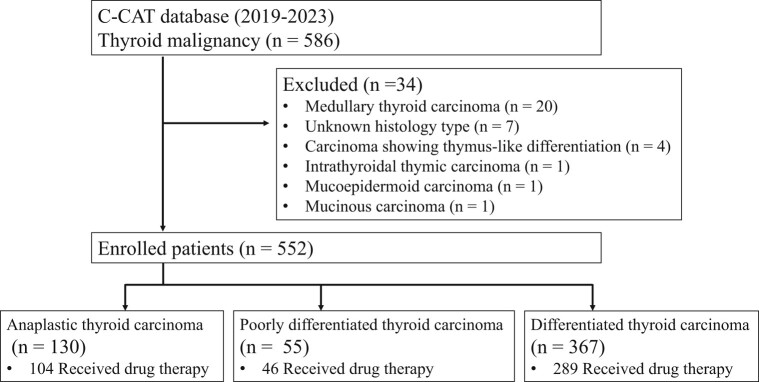
Methods: We conducted a retrospective observational study using a national database in Japan, which included 552 cases of thyroid carcinoma out of 53 543 patients in the database.
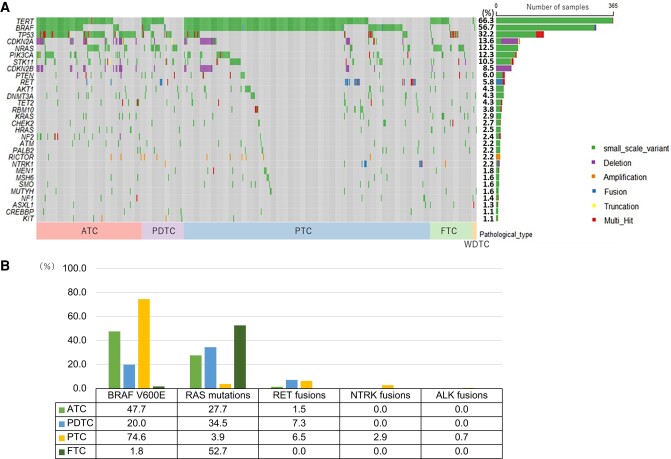
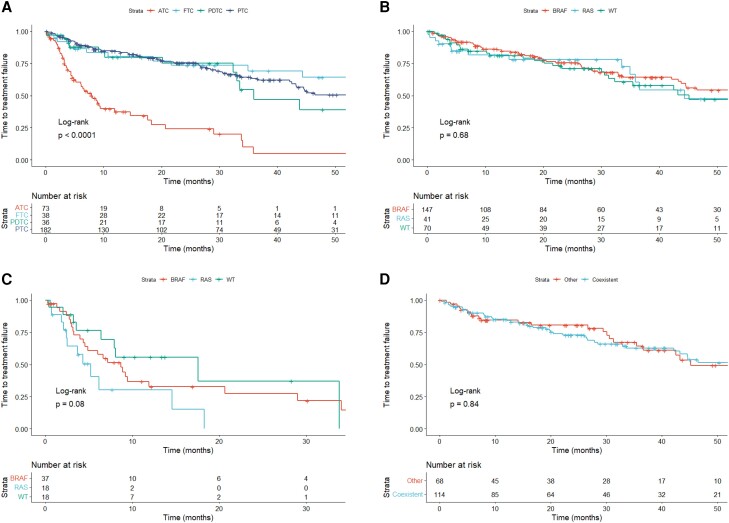
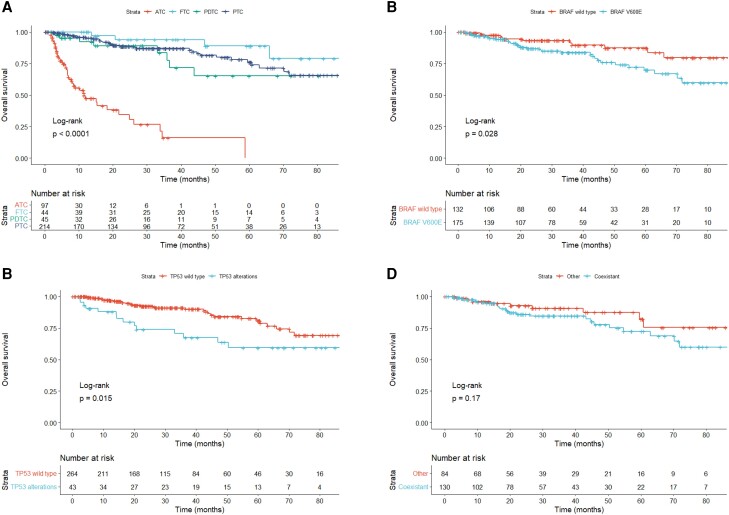
Results: The database included anaplastic thyroid carcinoma (23.6%), poorly differentiated thyroid carcinoma (10.0%), and differentiated thyroid carcinoma (66.4%). The most common genetic abnormalities were TERT promoter (66.3%), BRAF (56.7%), and TP53 (32.2%). The typical driver genes were BRAF V600E (55.0%), RAS (18.5%), RET fusion (4.7%), NTRK fusion (1.6%), and ALK fusion (0.4%). The most common regimen was lenvatinib, and the time to treatment failure was not different despite the presence of BRAF or RAS mutations. In differentiated thyroid carcinoma and poorly differentiated thyroid carcinoma, TP53 alterations independently predicted worse overall survival (hazard ratio = 2.205, 95% confidence interval: 1.135-4.283). In anaplastic thyroid carcinoma, no genetic alterations were associated with overall survival.
Conclusion: Genetic abnormalities with treatment options were found in 62.7% of advanced thyroid carcinomas. TP53 abnormality was an independent poor prognostic factor for overall survival in differentiated thyroid carcinoma. The time to treatment failure for lenvatinib was not different based on genetic profile.
Keywords: comprehensive genetic profiling test; fusions; gene; mutations; targeted therapy; thyroid carcinoma.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Molecular Pathology of Anaplastic Thyroid Carcinomas: A Retrospective Study of 144 Cases.Thyroid. 2017 May;27(5):682-692. doi: 10.1089/thy.2016.0254. Thyroid. 2017. PMID: 28351340
-
Comprehensive genomic profiling from C-CAT database unveiled over 80% presence of oncogenic drivers in anaplastic thyroid carcinoma including BRAF, RAS family, NF1, and FGFR1.Clin Endocrinol (Oxf). 2024 Aug;101(2):170-179. doi: 10.1111/cen.15098. Epub 2024 Jun 9. Clin Endocrinol (Oxf). 2024. PMID: 38853441
-
Real-World Experience with Targeted Therapy for the Treatment of Anaplastic Thyroid Carcinoma.Thyroid. 2018 Jan;28(1):79-87. doi: 10.1089/thy.2017.0285. Epub 2017 Dec 21. Thyroid. 2018. PMID: 29161986 Free PMC article.
-
A Narrative Review of Genetic Alterations in Primary Thyroid Epithelial Cancer.Int J Mol Sci. 2021 Feb 9;22(4):1726. doi: 10.3390/ijms22041726. Int J Mol Sci. 2021. PMID: 33572167 Free PMC article. Review.
-
Poorly Differentiated Carcinoma of the Thyroid Gland: Current Status and Future Prospects.Thyroid. 2019 Mar;29(3):311-321. doi: 10.1089/thy.2018.0509. Thyroid. 2019. PMID: 30747050 Free PMC article. Review.
Cited by
-
Concordance of BRAF V600E mutation between immunohistochemistry and genomic testing for thyroid cancer.Int J Clin Oncol. 2025 Jun;30(6):1143-1151. doi: 10.1007/s10147-025-02760-y. Epub 2025 Apr 10. Int J Clin Oncol. 2025. PMID: 40210835
-
Molecular predictive biomarker testing in advanced thyroid cancer - a European consensus.Eur Thyroid J. 2025 Jul 7;14(4):e250024. doi: 10.1530/ETJ-25-0024. Print 2025 Aug 1. Eur Thyroid J. 2025. PMID: 40540622 Free PMC article. Review.
-
Lenvatinib for unresectable anaplastic thyroid cancer: real-world experiences in multi-institutional study.Endocrine. 2025 Jun 28. doi: 10.1007/s12020-025-04333-5. Online ahead of print. Endocrine. 2025. PMID: 40581716
-
Cell cycle and HIF-1 related gene expression alteration in thyroid cell lines under microgravity.Oncol Res. 2025 Jul 18;33(8):1909-1931. doi: 10.32604/or.2025.065847. eCollection 2025. Oncol Res. 2025. PMID: 40746898 Free PMC article.
-
Anticancer drug therapy for anaplastic thyroid cancer.Eur Thyroid J. 2025 Apr 14;14(2):e240287. doi: 10.1530/ETJ-24-0287. Print 2025 Apr 1. Eur Thyroid J. 2025. PMID: 40163699 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
