Life-Threatening MOG Antibody-Associated Hemorrhagic ADEM With Elevated CSF IL-6
- PMID: 38630950
- PMCID: PMC11087044
- DOI: 10.1212/NXI.0000000000200243
Life-Threatening MOG Antibody-Associated Hemorrhagic ADEM With Elevated CSF IL-6
Abstract
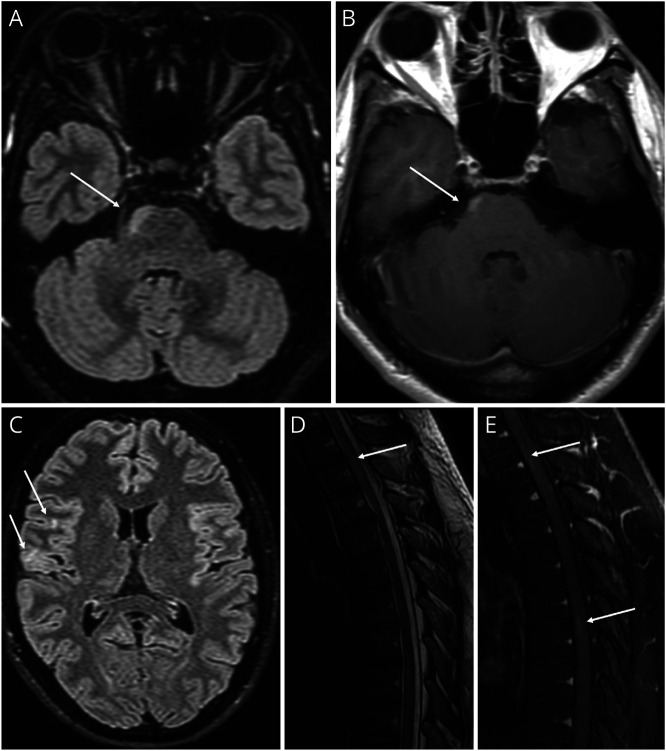
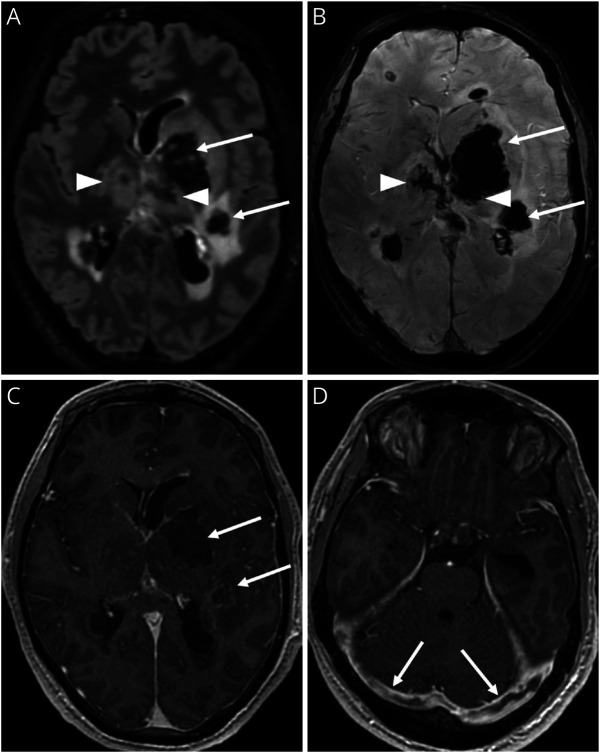
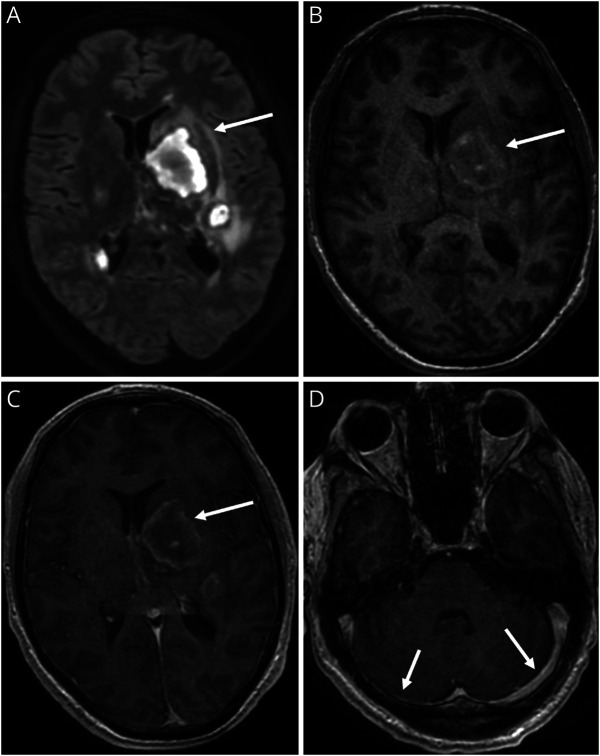
Acute disseminated encephalomyelitis (ADEM) is one characteristic manifestation of myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). A previously healthy man presented with retro-orbital headache and urinary retention 14 days after Tdap vaccination. Brain and spine MRI suggested a CNS demyelinating process. Despite treatment with IV steroids, he deteriorated, manifesting hemiparesis and later impaired consciousness, requiring intubation. A repeat brain MRI demonstrated new bilateral supratentorial lesions associated with venous sinus thrombosis, hemorrhage, and midline shift. Anti-MOG antibody was present at a high titer. CSF IL-6 protein was >2,000 times above the upper limits of normal. He improved after plasma exchange, then began monthly treatment alone with anti-IL-6 receptor antibody, tocilizumab, and has remained stable. This case highlights how adult-onset MOGAD, like childhood ADEM, can rapidly become life-threatening. The markedly elevated CSF IL-6 observed here supports consideration for evaluating CSF cytokines more broadly in patients with acute MOGAD.
Conflict of interest statement
A. Virupakshaiah is supported by fellowship support from Biogen, EMD Serono and Novartis. C.E. Moseley is supported by a National Multiple Sclerosis Society Clinician Scientist Development Award # FAN-2107-38301. S.S. Zamvil is supported by NIH grants 1 R01 AI131624-01A1 and 1 RO1 AI170863-01A1. All other authors report no disclosures relevant to the manuscript. Go to
Figures