

De Novo Brain Vascular Malformations in Hereditary Hemorrhagic Telangiectasia
- PMID: 38631080
- PMCID: PMC11102835
- DOI: 10.1016/j.pediatrneurol.2024.03.013
De Novo Brain Vascular Malformations in Hereditary Hemorrhagic Telangiectasia
Abstract
Background: Approximately 10% of people with hereditary hemorrhagic telangiectasia (HHT) have brain vascular malformations (VMs). Few reports describe de novo brain VM formation. International HHT Guidelines recommend initial brain VM screening upon HHT diagnosis in children but do not address rescreening. We aimed to confirm whether brain VMs can form de novo in patients with HHT.
Methods: The Brain Vascular Malformation Consortium HHT project is a 17-center longitudinal study enrolling patients since 2010. We analyzed the database for de novo VMs defined as those detected (1) on follow-up neuroimaging in a patient without previous brain VMs or (2) in a location distinct from previously identified brain VMs and reported those in whom a de novo VM could be confirmed on central neuroimaging review.
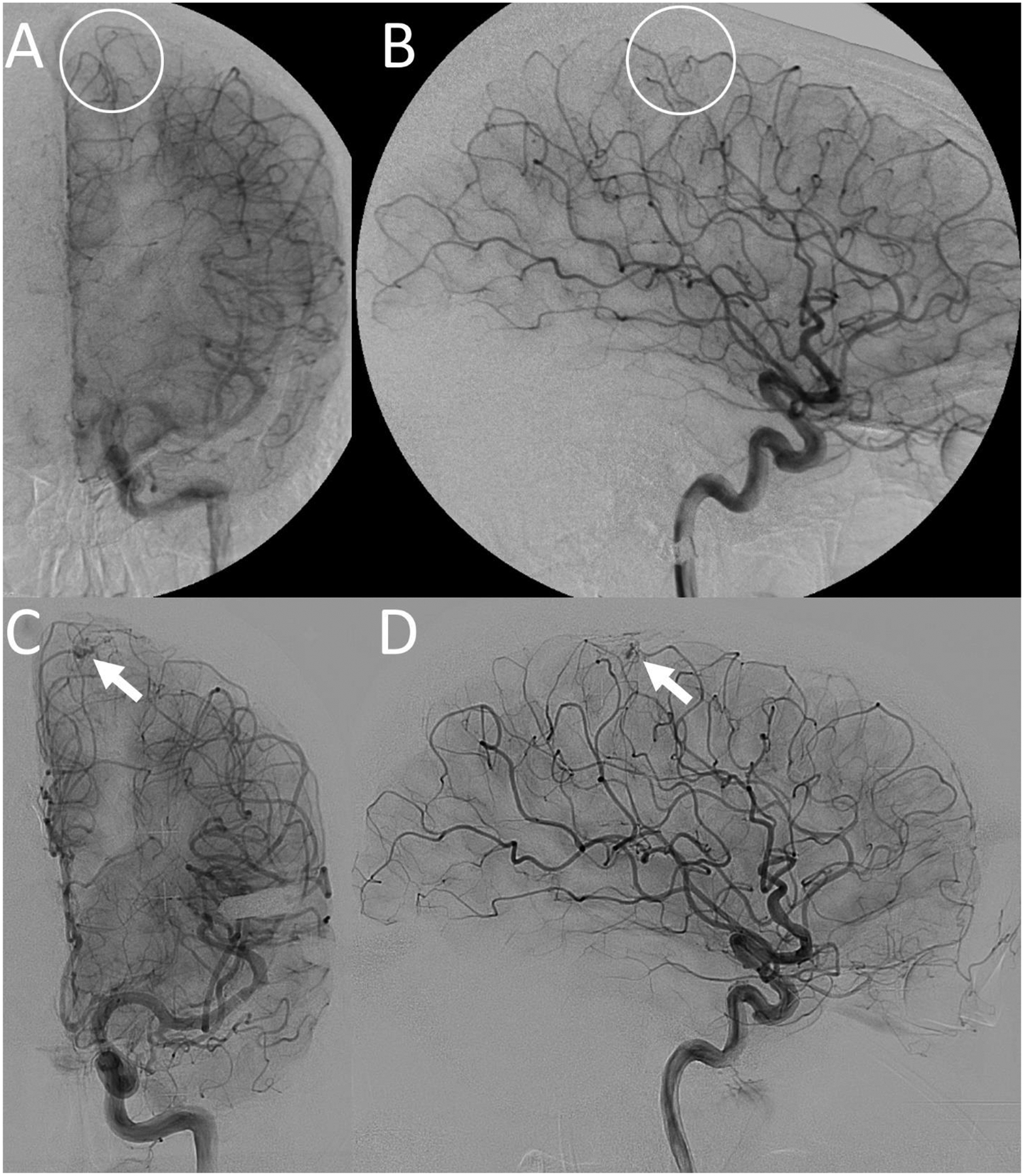
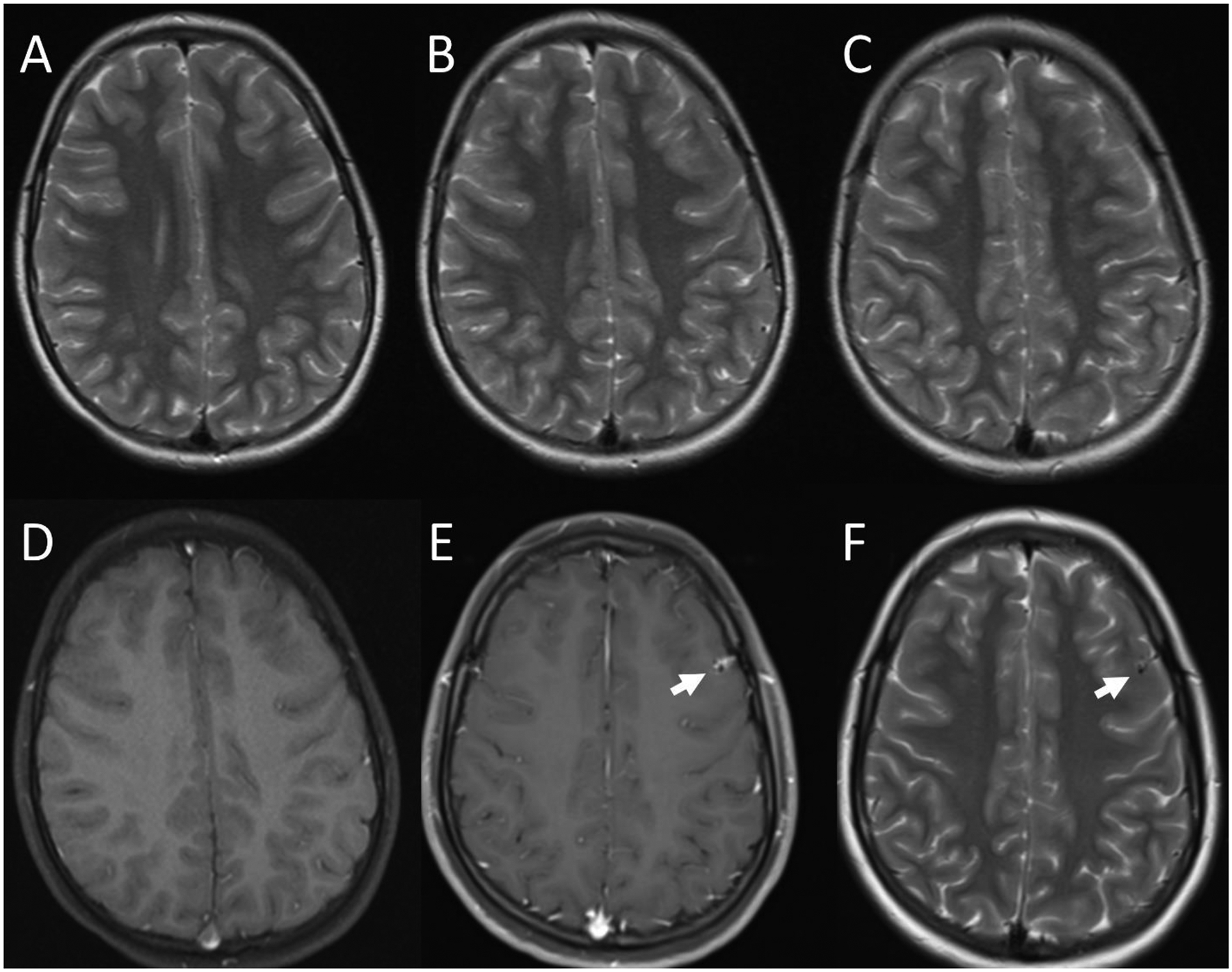
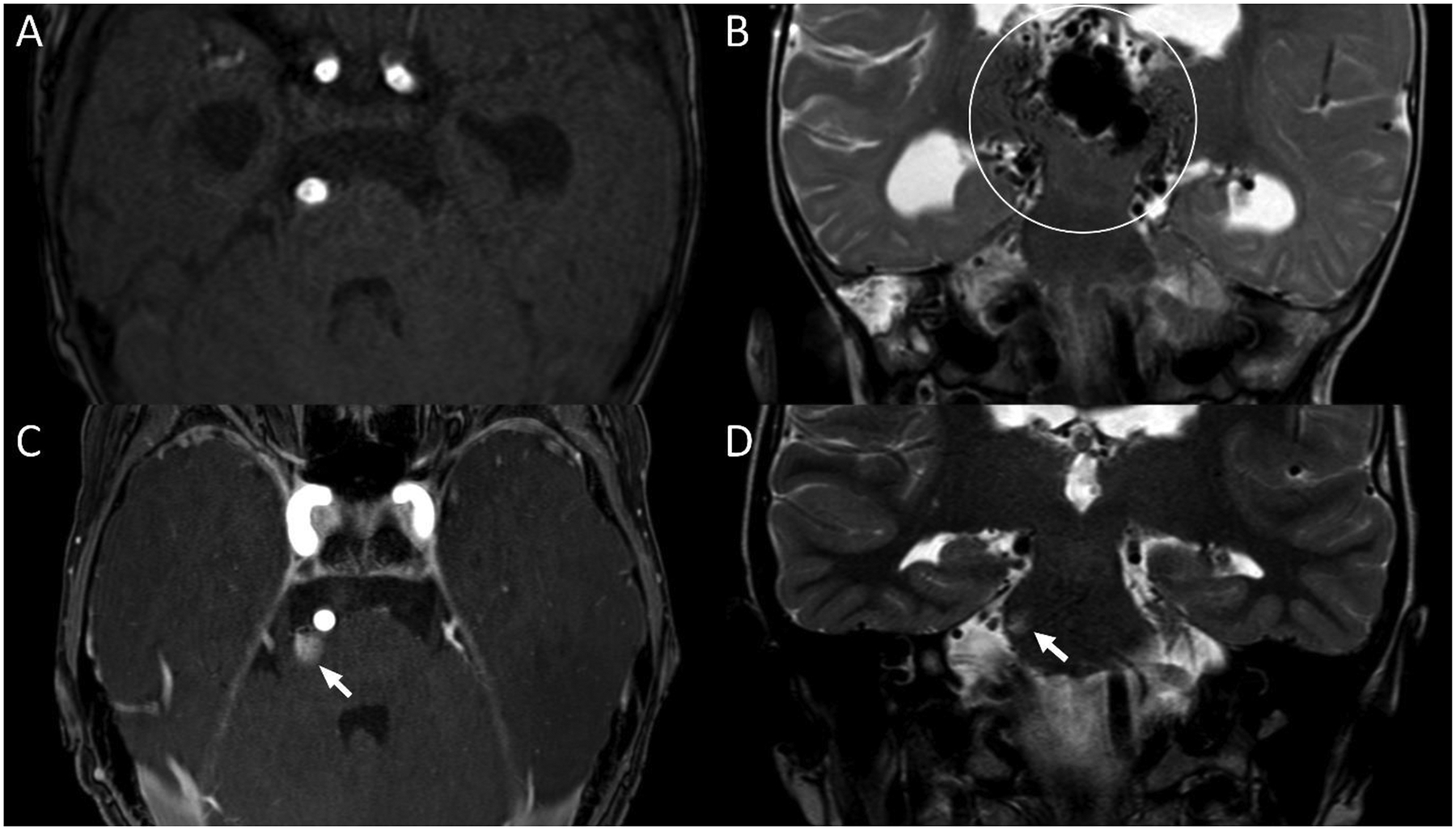
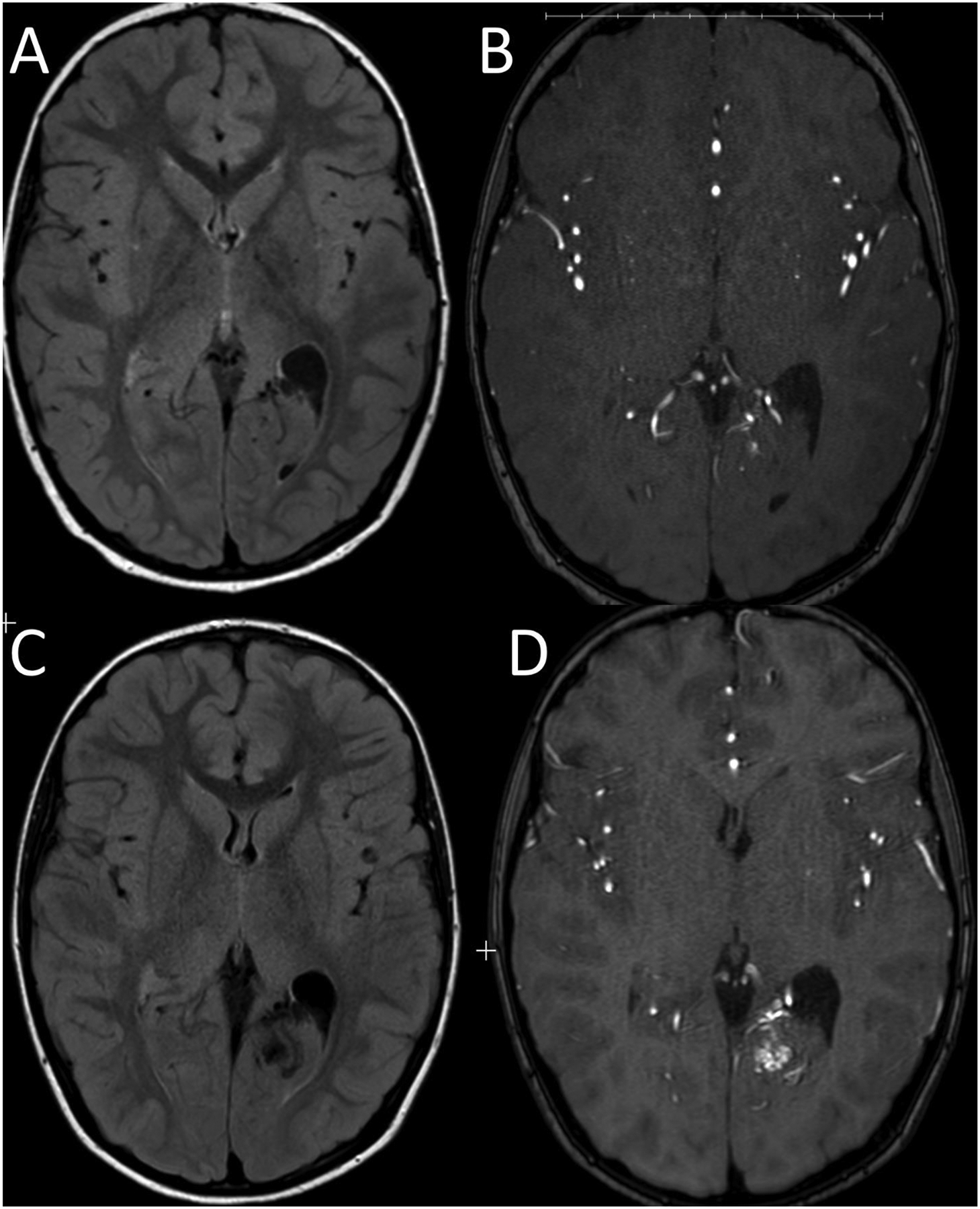
Results: Of 1909 patients enrolled, 409 (21%) had brain VMs. Seven patients were recorded as having de novo brain VMs, and imaging was available for central review in four. We confirmed that three (0.7% of individuals with brain VMs) had de novo brain VMs (two capillary malformations, one brain arteriovenous malformation) with intervals of six, nine, and 13 years from initial imaging. Two with de novo brain VMs were <18 years. The fourth patient, a child, did not have a de novo brain VM but had a radiologically confirmed increase in size of an existing brain arteriovenous malformation.
Conclusions: Brain VMs can, albeit rarely, form de novo in patients with HHT. Given the potential risk of hemorrhage from brain VMs, regular rescreening in patients with HHT may be warranted.
Keywords: Brain arteriovenous malformation; Brain vascular malformation; Capillary malformation; De novo; Hereditary hemorrhagic telangiectasia.
Copyright © 2024 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The Brain Vascular Malformation Consortium (U54NS065705) is a part of the NCATS Rare Diseases Clinical Research Network (RDCRN) and is supported by the RDCRNData Management and Coordinating Center (DMCC) (U2CTR002818). RDCRN is an initiative of the Office of Rare Diseases Research (ORDR), NCATS, funded through a collaboration between NCATS and NINDS. L.A.B. was supported by a BVMC fellowship, as part of the funding detailed above. L.A.B. was also supported by the Children's Hospital of Philadelphia Department of Pediatrics Chair's Initiative. M.E.F. was also supported by the Li Ka Shing Knowledge Institute. None of the funding sources directly participated in the study design, data collection, analysis and interpretation of data, writing of the report, or the decision to submit the article for publication.
Figures
References
-
- McDonald J, Bayrak-Toydemir P, DeMille D, Wooderchak-Donahue W, Whitehead K. Curaçao diagnostic criteria for hereditary hemorrhagic telangiectasia is highly predictive of a pathogenic variant in ENG or ACVRL1 (HHT1 and HHT2) Genet Med 2020;22(7):1201–1205. DOI: 10.1038/s41436-;020-0775-;8 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
