

Long-Term Healthcare Resource Utilization and Costs among Patients with Myasthenia Gravis: A Swedish Nationwide Population-Based Study
- PMID: 38631321
- PMCID: PMC11633887
- DOI: 10.1159/000538640
Long-Term Healthcare Resource Utilization and Costs among Patients with Myasthenia Gravis: A Swedish Nationwide Population-Based Study
Abstract
Introduction: Healthcare costs and societal impact of myasthenia gravis (MG), a potentially life-threatening rare, chronic neuromuscular disease, are sparsely studied. We assessed healthcare resource utilization (HCRU) and associated costs among patients with newly diagnosed (ND) and preexisting (PE) MG in Sweden.
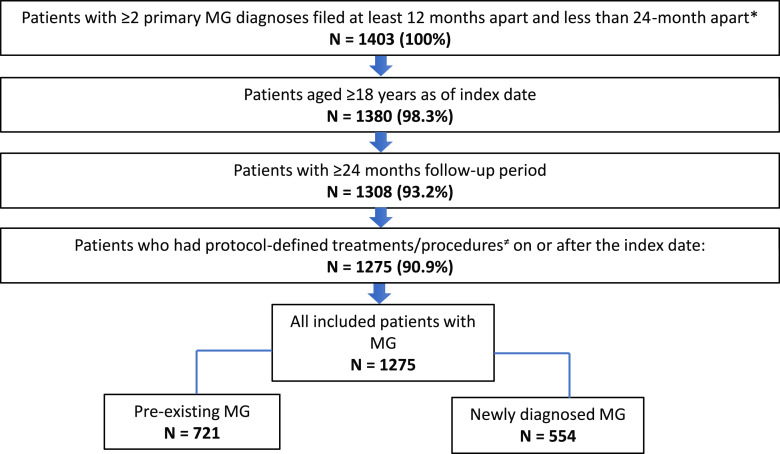
Methods: This observational, retrospective cohort study used data from four linkable Swedish nationwide population-based registries. Adult MG patients receiving pharmacological treatment for MG and having ≥24-month follow-up during the period January 1, 2010, to December 31, 2017, were included.
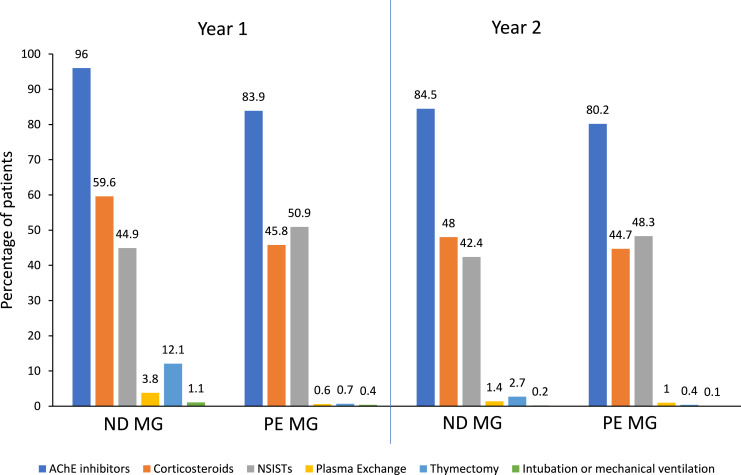
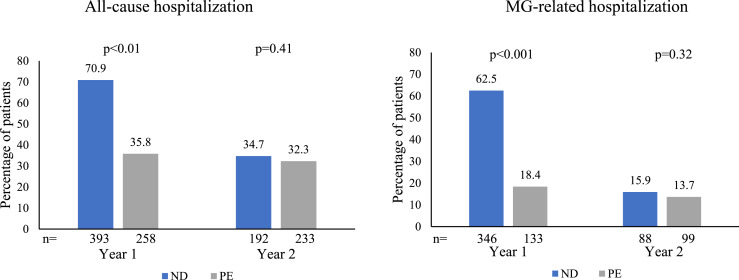
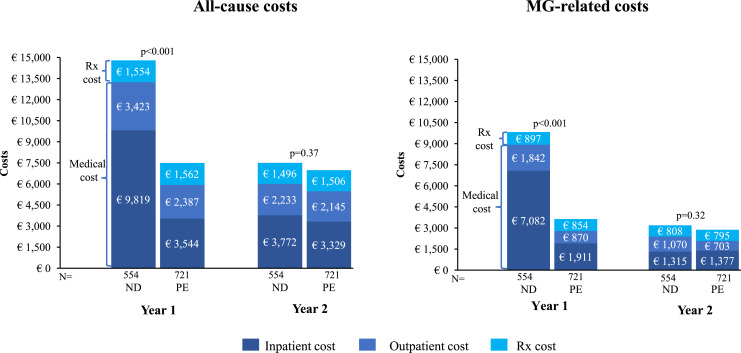
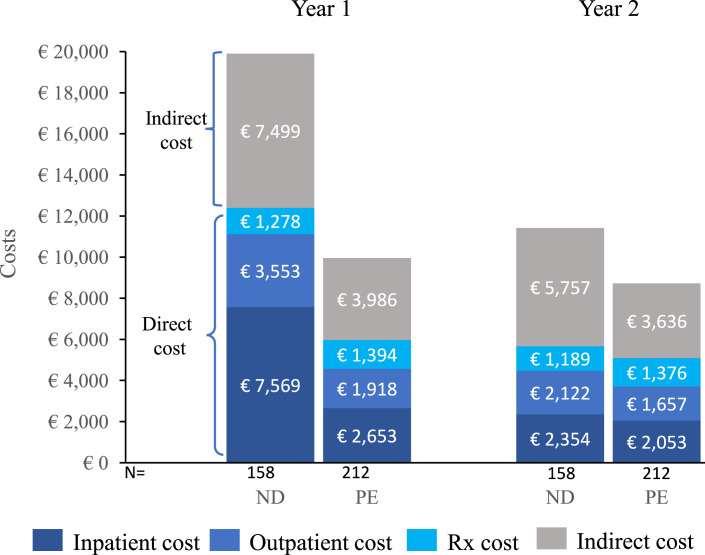
Results: A total of 1,275 patients were included in the analysis, of which 554 patients were categorized into the ND MG group and 721 into the PE MG group. Mean (±SD) age was 61.3 (±17.4) years, and 52.3% were female. In the first year post-diagnosis, ND patients had significantly higher utilization of acetylcholinesterase inhibitors (96.0% vs. 83.9%), corticosteroids (59.6% vs. 45.8%), thymectomy (12.1% vs. 0.7%), and plasma exchange (3.8% vs. 0.6%); had higher all-cause (70.9% vs. 35.8%) and MG-related (62.5% vs. 18.4%) hospitalization rates with 11 more hospitalization days (all p < 0.01) and an increased risk of hospitalization (odds ratio [95% CI] = 4.4 [3.43, 5.64]) than PE MG. In year 1 post-diagnosis, ND MG patients incurred EUR 7,302 (p < 0.01) higher total all-cause costs than PE MG, of which 84% were estimated to be MG-related and the majority (86%) were related to inpatient care. These results remained significant also after controlling for baseline demographics and comorbidities (p < 0.01). In year 2 post-diagnosis, the all-cause medical costs decreased by ∼55% for ND MG from year 1 and were comparable with PE MG.
Conclusion: In this population-based study, MG patients required significantly more healthcare resources in year 1 post-diagnosis than PE MG primarily due to more pharmacological treatments, thymectomies, and associated hospitalizations. These findings highlight the need to better understand potential factors including disease characteristics associated with increased health resource use and costs and need for more efficacious treatments early in the disease course.
Keywords: Healthcare costs; Myasthenia gravis; Resource utilization; Sickness absence.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Qian Cai, Alberto E. Batista, Qiaoyi Zhang, Peter Kunovszki, Kavita Gandhi, and Kristin Heerlein are employees of Janssen Pharmaceuticals and may hold stock or stock options in Johnson & Johnson. Jakob Börsum was employed by SDS Life Science AB, Uppsala, Sweden. Gabriel Isheden owns 100% of the shares of Intelligent Decision Analytics AB and was contracted with SDS Life Science AB to carry out work for this manuscript. Susanna Brauner received grants from UCB Pharma outside the submitted work.
Figures
Similar articles
-
Economic and societal burden of myasthenia gravis in Denmark, Finland, and Sweden: A population-based registry study.Eur J Neurol. 2024 Dec;31(12):e16511. doi: 10.1111/ene.16511. Epub 2024 Oct 9. Eur J Neurol. 2024. PMID: 39380430 Free PMC article.
-
Health care costs and resource utilization among patients with myasthenia gravis in the United States.J Manag Care Spec Pharm. 2025 May;31(5):472-481. doi: 10.18553/jmcp.2025.31.5.472. J Manag Care Spec Pharm. 2025. PMID: 40298306 Free PMC article.
-
Economic burden of generalized myasthenia gravis (MG) in the United States and the impact of common comorbidities and acute MG-events.Curr Med Res Opin. 2024 Jul;40(7):1145-1153. doi: 10.1080/03007995.2024.2353381. Epub 2024 May 24. Curr Med Res Opin. 2024. PMID: 38745448
-
Healthcare resource utilization by patients with treatment-refractory myasthenia gravis in England.J Med Econ. 2019 Jul;22(7):691-697. doi: 10.1080/13696998.2019.1592180. Epub 2019 Mar 29. J Med Econ. 2019. PMID: 30841772
-
Healthcare Resource Utilization (HCRU) and Direct Medical Costs Associated with Long COVID or Post-COVID-19 Conditions: Findings from a Literature Review.J Mark Access Health Policy. 2025 Feb 12;13(1):7. doi: 10.3390/jmahp13010007. eCollection 2025 Mar. J Mark Access Health Policy. 2025. PMID: 39990183 Free PMC article. Review.
Cited by
-
Costs of Neurological Disorders.Neuroepidemiology. 2024;58(6):409-411. doi: 10.1159/000539370. Epub 2024 May 22. Neuroepidemiology. 2024. PMID: 38768584 Free PMC article. No abstract available.
-
Economic and societal burden of myasthenia gravis in Denmark, Finland, and Sweden: A population-based registry study.Eur J Neurol. 2024 Dec;31(12):e16511. doi: 10.1111/ene.16511. Epub 2024 Oct 9. Eur J Neurol. 2024. PMID: 39380430 Free PMC article.
-
Understanding symptoms in the lives of adult patients with acute or chronic illness: a phenomenological study of patient experiences.Int J Qual Stud Health Well-being. 2025 Dec;20(1):2534871. doi: 10.1080/17482631.2025.2534871. Epub 2025 Jul 30. Int J Qual Stud Health Well-being. 2025. PMID: 40736357 Free PMC article.
-
The economic burden of Myasthenia gravis from the patient´s perspective and reflected in German claims data.Sci Rep. 2025 Feb 25;15(1):6687. doi: 10.1038/s41598-025-91372-7. Sci Rep. 2025. PMID: 39994434 Free PMC article.
References
-
- Gilhus NE, Tzartos S, Evoli A, Palace J, Burns TM, Verschuuren JJGM. Myasthenia gravis. Nat Rev Dis Primers. 2019;5(1):30. - PubMed
-
- Jaretzki A, Kaminski HJ, Keesey JC, Penn AS, Barohn RJ, Ernstoff RM, et al. . Myasthenia gravis: recommendations for clinical research standards. Task force of the medical scientific advisory board of the myasthenia gravis foundation of America. Neurology. 2000;55(1):16–23. - PubMed
-
- Beloor Suresh A, Asuncion RMD. Myasthenia Gravis. StatPearls. Treasure Island (FL) relationships with ineligible companies. Disclosure: Ria Monica Asuncion declares no relevant financial relationships with ineligible companies: StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC., 2023.
-
- Gilhus NE. Myasthenia gravis. N Engl J Med. 2016;375(26):2570–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
