

Defining predictors of responsiveness to advanced therapies in Crohn's disease and ulcerative colitis: protocol for the IBD-RESPONSE and nested CD-metaRESPONSE prospective, multicentre, observational cohort study in precision medicine
- PMID: 38631839
- PMCID: PMC11029295
- DOI: 10.1136/bmjopen-2023-073639
Defining predictors of responsiveness to advanced therapies in Crohn's disease and ulcerative colitis: protocol for the IBD-RESPONSE and nested CD-metaRESPONSE prospective, multicentre, observational cohort study in precision medicine
Abstract
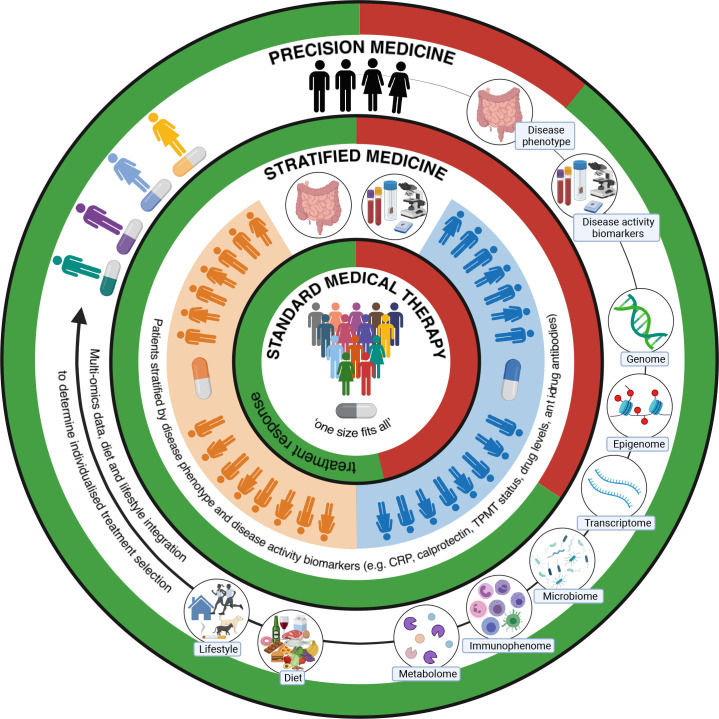
Introduction: Characterised by chronic inflammation of the gastrointestinal tract, inflammatory bowel disease (IBD) symptoms including diarrhoea, abdominal pain and fatigue can significantly impact patient's quality of life. Therapeutic developments in the last 20 years have revolutionised treatment. However, clinical trials and real-world data show primary non-response rates up to 40%. A significant challenge is an inability to predict which treatment will benefit individual patients.Current understanding of IBD pathogenesis implicates complex interactions between host genetics and the gut microbiome. Most cohorts studying the gut microbiota to date have been underpowered, examined single treatments and produced heterogeneous results. Lack of cross-treatment comparisons and well-powered independent replication cohorts hampers the ability to infer real-world utility of predictive signatures.IBD-RESPONSE will use multi-omic data to create a predictive tool for treatment response. Future patient benefit may include development of biomarker-based treatment stratification or manipulation of intestinal microbial targets. IBD-RESPONSE and downstream studies have the potential to improve quality of life, reduce patient risk and reduce expenditure on ineffective treatments.
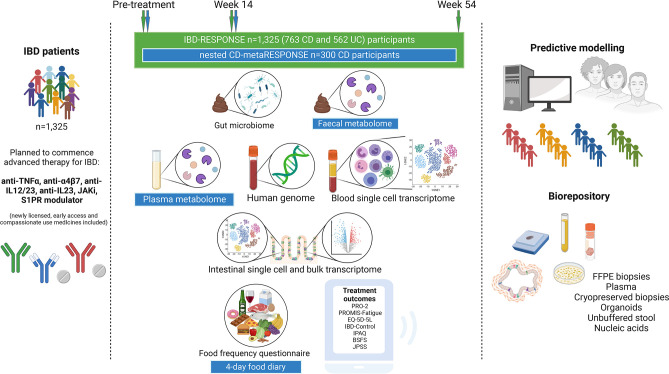
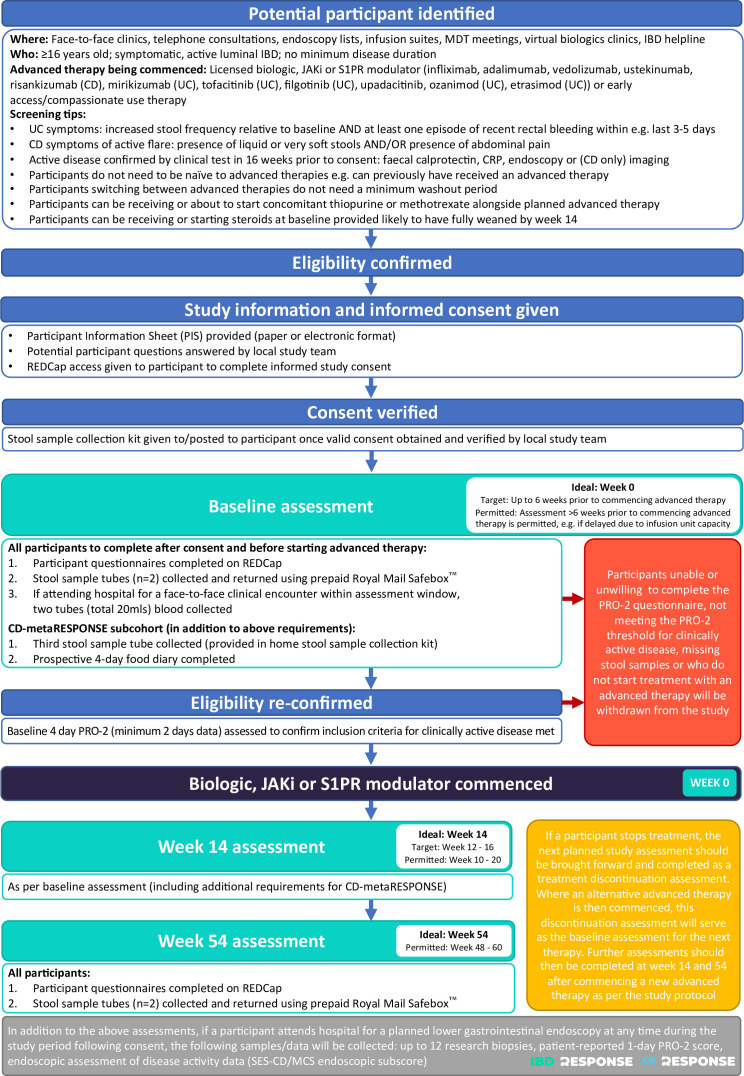
Methods and analysis: This prospective, multicentre, observational study will identify and validate a predictive model for response to advanced IBD therapies, incorporating gut microbiome, metabolome, single-cell transcriptome, human genome, dietary and clinical data. 1325 participants commencing advanced therapies will be recruited from ~40 UK sites. Data will be collected at baseline, week 14 and week 54. The primary outcome is week 14 clinical response. Secondary outcomes include clinical remission, loss of response in week 14 responders, corticosteroid-free response/remission, time to treatment escalation and change in patient-reported outcome measures.
Ethics and dissemination: Ethical approval was obtained from the Wales Research Ethics Committee 5 (ref: 21/WA/0228). Recruitment is ongoing. Following study completion, results will be submitted for publication in peer-reviewed journals and presented at scientific meetings. Publications will be summarised at www.ibd-response.co.uk.
Trial registration number: ISRCTN96296121.
Keywords: gastroenterology; inflammatory bowel disease; microbiology; patient reported outcome measures; patient-centered care.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: TA reports personal grants from F. Hoffmann-La Roche, Biogen, AbbVie, Janssen, Celltrion, Galapagos, Immunodiagnostik and Takeda, outside the submitted work; personal fees for educational development/delivery from Pfizer, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Pfizer, Takeda and F. Hoffman-La Roche; support for attending meetings from Celltrion, Tillotts and Pfizer. CAA reports grants from the Wellcome Sanger Institute Quinquennial Review 2021–2026, Crohn’s and Colitis Foundation (USA), the Medical Research Council, Open Targets UK and the Helmsley Charitable Trust; consulting fees from BridgeBio, Genomics and Brigham & Women’s Hospital Boston; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from GlaxoSmithKline; support for attending meetings and/or travel membership from the Wellcome Sanger Institute Quinquennial Review 2021–2026; (Chair) of the Board of Trustees for the Sanger Prize; other interests as Director of Anderson Genomics Consultancy. MB reports partial personal salary funding from the Medical Research Council. ALH reports personal consulting fees from AbbVie, BMS, Celltrion, Falk, Galapagos, Janssen, Pfizer, Takeda and Roche; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from BMS, Celltrion, Falk, Galapagos, Janssen, Pfizer, Takeda, Roche and AbbVie; support for attending meetings and/or travel from BMS, Celltrion, Falk, Galapagos, Janssen, Pfizer, Takeda, Roche and AbbVie. PI reports personal grants from Celltrion, Galapagos and Pfizer, outside the submitted work; personal consulting fees from AbbVie, Takeda, BMS, Janssen, Arena, Pfizer, Galapagos, Lilly, Boehringer-Ingelheim and Celgene; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Takeda, Janssen, Lilly, BMS, Pfizer and Galapagos; support for attending meetings and/or travel from AbbVie and Tillotts. LJ-D reports grants from the Wellcome Trust, the Royal Society, the Kennedy Trust for Rheumatology Research, the Helmsley Charitable Trust and the Medical Research Council; grants from Novartis Pharmaceutical, outside the submitted work; consulting fees from Nightingale Health and Genomics. CK reports partial salary funding from the Medical Research Council. NAK reports grants from AbbVie, Biogen, Celltrion, Galapagos and Immunodiagnostik; consulting fees from AbbVie, Bristol-Meyers Squibb and Dr Falk; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Dr Falk, Tillotts, Galapagos and Takeda; support for attending meetings and/or travel from Tillotts; participation (Chair) on the Board of the British Society of Gastroenterology IBD Clinical Research Group. CAL reports grants from and/or consultancy for Janssen, Takeda, AbbVie, AstraZeneca, Eli Lilly, Orion, Pfizer, Roche, Sanofi Aventis, UCB, Biogen, GSK, Bristol-Myers Squibb and Genentech; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Ferring, Takeda, Janssen, Nordic Pharma and Dr Falk; participation (Secretary) on the British Society of Gastroenterology IBD Section; participation on the Steering Committee of IBD UK. CWL reports grants from UKRI Future Leaders Fellowship; personal consulting fees from AbbVie, Pfizer, Janssen, Takeda, Galapagos, Fresnius Kabi, Novartis/Sandoz, BMS and Celltrion; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Pfizer, Janssen, Takeda, Galapagos, Fresnius Kabi, Novartis/Sandoz, BMS, Ferring, Dr Falk and Celltrion. JOL reports grants from AbbVie, and Gilead; personal consulting fees from Allergan, AbbVie, Bristol-Myers Squibb, Celgene, Cornerstones US, Galapagos, Gilead, GSK, Lilly, MSD UK, Shire UK, Shire International, Ferring UK, Ferring International, Celltrion, Takeda, Pfizer and Janssen; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Bristol-Myers Squibb, Cornerstones US, Galapagos, Ferring UK, Ferring International, Celltrion, Takeda, Pfizer and Janssen; support to attend meetings and/or travel from AbbVie and Janssen. RHM reports that she is an independent membership on the Trial Steering Committee for the National Institute for Health and Care Research funded ALLEGRO trial. JRM reports personal consulting fees from EnteroBiotix and Cultech; patent held (without financial gain) on Clostridium difficile therapy (WO2019197836A1), participation (Chair) on the IDMC Board. NMcG reports partial (10%) salary funding from the Medical Research Council. REM reports personal salary funding from the Wellcome Sanger Institute. JO reports stock held in Novartis. MP reports grants from Pfizer and Gilead; personal consulting fees from Galapagos; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen. NP reports grants from Bristol-Myers Squibb, Takeda and Pfizer; consulting fees from AbbVie, Allergan, AstraZeneca, Bristol-Myers Squibb, Celgene, Celltrion, Galapagos, GSK, Takeda and Vifor; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Bristol-Myers Squibb, Ferring, Galapagos, Janssen, Roche, Pfizer, Takeda and Tillotts; support for attending meetings and/or travel from AbbVie, Allergan, Celltrion, Janssen and Takeda; participation on a data safety monitoring board or advisory board for AbbVie, Allergan, AstraZeneca, Bristol-Myers Squibb, Celgene, Celltrion, Galapagos, GSK, Takeda and Vifor. TR reports personal grants from AbbVie; personal consulting fees from AbbVie, Arena, Aslan, AstraZeneca, Boehringer-Ingelheim, BMS, Celgene, Ferring, Galapagos, Gilead, GSK, Heptares, LabGenius, Janssen, Mylan, MSD, Novartis, Pfizer, Roche, Sandoz, Takeda, UCB and XAP therapeutics; participation on the board of UCB, membership (Chair) of the ECCO Guidelines Committee, membership of the UEG Scientific Committee. JS reports grants from Crohn’s and Colitis UK, the Helmsley Charitable Trust, ECCO, the European Commission, CCFA and Action Medical Research; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Roche; participation on a Data Safety Monitoring Board or Advisory Board for the MODULATE trial and the TRIBUTE trial; leadership or fiduciary role as the Director of the Royal College of Physicians IBD Registry, and Governing Body Fellow at Green Templeton College. AS reports personal consulting fees from GSK; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Falk, and AbbVie; payment of conference fees to attend the British Society of Gastroenterology Annual Conference 2022 from Celltrion; participation on a Data Safety Monitoring Board or Advisory Board for the IBD-RESPONSE study (unpaid), and AbbVie; participation on the British Society of Gastroenterology IBD Section Committee. CJS reports personal consultancy fees from Astarte Medical; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Nestle Nutrition Institute. JW reports grants from Intercept; consulting fees from Worg and UCB; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen; participation on a Data Safety Monitoring Board or Advisory Board for Roche. KW reports grants from the Helsmsley Charitable Trust, Crohn’s and Colitis UK, Almond Board of California, Danone, International Dried Fruit and Nut Council, Medical Research Council, National Institute for Health and care Research; royalty or license payments for Volatile organic compounds in the diagnosis and management of irritable bowel syndrome, and Wiley BDA Advances in Nutrition & Dietetics book series; personal consulting fees from Danone; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen; support for attending meetings and/or travel from Yakult; participation on a Data Safety Monitoring Board or Advisory Board for the MODULATE trial (unpaid).
Figures
References
-
- van der Valk ME, Mangen M-JJ, Leenders M, et al. . Risk factors of work disability in patients with inflammatory bowel disease--a Dutch nationwide web-based survey: work disability in inflammatory bowel disease. J Crohns Colitis 2014;8:590–7.:S1873-9946(13)00408-X. 10.1016/j.crohns.2013.11.019 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical