

Pancreatic head resection for carcinoma of the ampulla vateri - better long-term prognosis, but more postoperative complications
- PMID: 38632147
- PMCID: PMC11024026
- DOI: 10.1007/s00423-024-03319-7
Pancreatic head resection for carcinoma of the ampulla vateri - better long-term prognosis, but more postoperative complications
Abstract
Background: Pancreatoduodenectomies are complex surgical procedures with a considerable morbidity and mortality even in high-volume centers. However, postoperative morbidity and long-term oncological outcome are not only affected by the surgical procedure itself, but also by the underlying disease. The aim of our study is an analysis of pancreatoduodenectomies for patients with pancreatic ductal adenocarcinoma (PDAC) and ampullary carcinoma (CAMP) concerning postoperative complications and long-term outcome in a tertiary hospital in Germany.
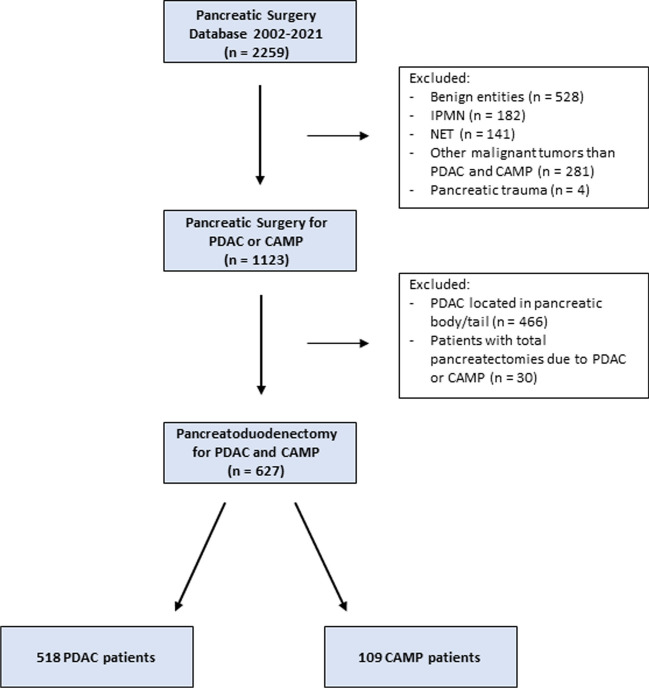
Methods: The perioperative and oncological outcome of 109 pancreatic head resections performed for carcinoma of the ampulla vateri was compared to the outcome of 518 pancreatic head resections for pancreatic ductal adenocarcinoma over a 20 year-period from January 2002 until December 2021. All operative procedures were performed at the University Hospital Freiburg, Germany. Patient data was analyzed retrospectively, using a prospectively maintained SPSS database. Propensity score matching was performed to adjust for differences in surgical and reconstruction technique. Primary outcome of our study was long-term overall survival, secondary outcomes were postoperative complications and 30-day postoperative mortality. Postoperative complications like pancreatic fistula (POPF), postpancreatectomy hemorrhage (PPH) and delayed gastric emptying (DGE) were graded following current international definitions. Survival was estimated using Kaplan Meier curves and log-rank tests. A p-value < 0.05 was considered statistically significant.
Results: Operation time was significantly longer in PDAC patients (432 vs. 391 min, p < 0.001). The rate of portal vein resections was significantly higher in PDAC patients (p < 0.001). In CAMP patients, a pancreatogastrostomy as reconstruction technique was performed more frequently compared to PDAC patients (48.6% vs. 29.9%, p < 0.001) and there was a trend towards more laparoscopic surgeries in CAMP patients (p = 0.051). After propensity score matching, we found no difference in DGE B/C and PPH B/C (p = 0.389; p = 0.517), but a significantly higher rate of clinically relevant pancreatic fistula (CR-POPF) in patients with pancreatoduodenectomies due to ampullary carcinoma (30.7% vs. 16.8%, p < 0.001). Long-term survival was significantly better in CAMP patients (42 vs. 24 months, p = 0.003).
Conclusion: Patients with pancreatoduodenectomies due to ampullary carcinomas showed a better long-term oncological survival, by reason of the better prognosis of this tumor entity. However, these patients often needed a more elaborated postoperative treatment due to the higher rate of clinically relevant pancreatic fistula in this group.
Keywords: Oncological outcome; Pancreatic cancer - ampullary carcinoma; Pancreatoduodenectomy; Postoperative complications.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
