

Conditional survival and annual hazard of death in older patients with esophageal cancer receiving definitive chemoradiotherapy
- PMID: 38632503
- PMCID: PMC11025141
- DOI: 10.1186/s12877-024-04939-w
Conditional survival and annual hazard of death in older patients with esophageal cancer receiving definitive chemoradiotherapy
Abstract
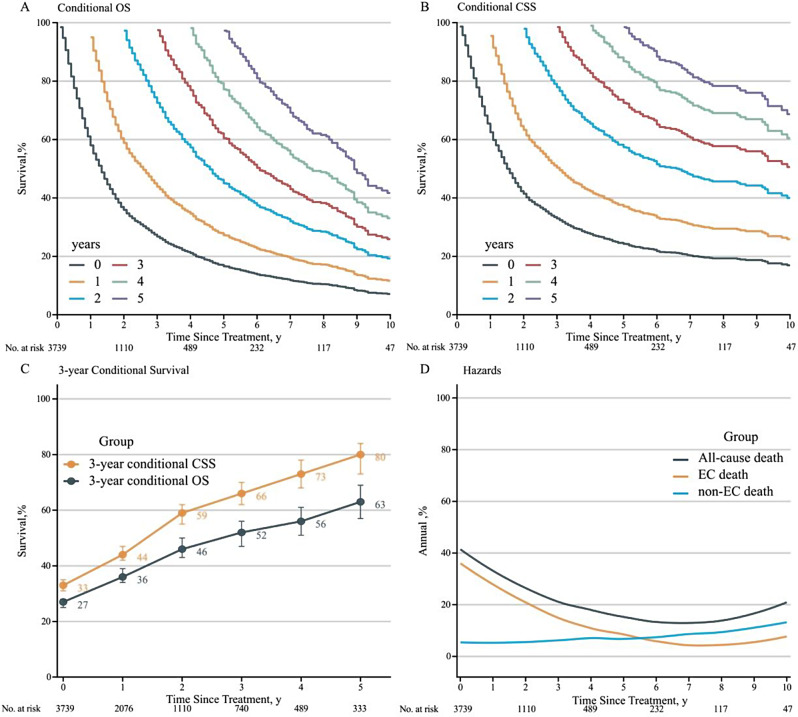
Background: Definitive chemoradiotherapy is one of the primary treatment modalities for older patients with esophageal cancer (EC). However, the evolution of prognosis over time and the factors affected non-EC deaths remain inadequately studied. We examined the conditional survival and annual hazard of death in older patients with EC after chemoradiotherapy.
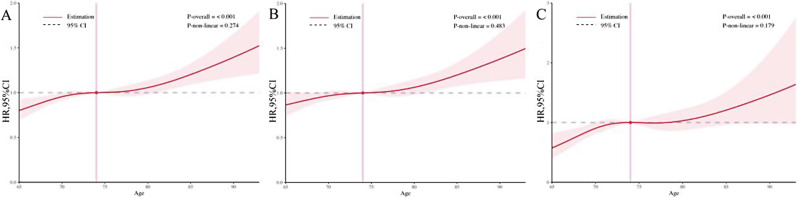
Methods: We collected data from patients aged 65 or older with EC registered in the Surveillance, Epidemiology, and End Results database during 2000-2019. Conditional survival was defined as the probability of survival given a specific time survived. Annual hazard of death was defined the yearly event rate. Restricted cubic spline (RCS) analysis identified the association of age at diagnosis with mortality.
Results: Among 3739 patients, the 3-year conditional overall survival increased annually by 7-10%. Non-EC causes accounted for 18.8% of deaths, predominantly due to cardio-cerebrovascular diseases. The hazard of death decreased from 40 to 10% in the first 6 years and then gradually increased to 20% in the tenth year. Non-EC causes surpassed EC causes in hazard starting 5 years post-treatment. RCS indicated a consistent increase in death hazard with advancing age, following a linear relationship. The overall cohort was divided into two groups: 65-74 and ≥ 75 years old, with the ≥ 75-year-old group showing poorer survival and earlier onset of non-EC deaths (HR = 1.36, 95% CI: 1.15-1.62, P < 0.001). Patients with early-stage disease (I-II) had higher risks of death from non-EC causes (HR = 0.82, 95% CI: 0.68-0.98, P = 0.035). Tumor histology had no significant impact on non-EC death risk (HR = 1.17, 95% CI: 0.98-1.39, P = 0.081).
Conclusions: Survival probability increases with time for older patients with EC treated with chemoradiotherapy. Clinicians and patients should prioritize managing and preventing age-related comorbidities, especially in older cohorts and those with early-stage disease.
Keywords: Conditional survival; Death hazard; Esophageal cancer; Older.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
