

The Brain Gene Registry: a data snapshot
- PMID: 38632549
- PMCID: PMC11022437
- DOI: 10.1186/s11689-024-09530-3
The Brain Gene Registry: a data snapshot
Abstract
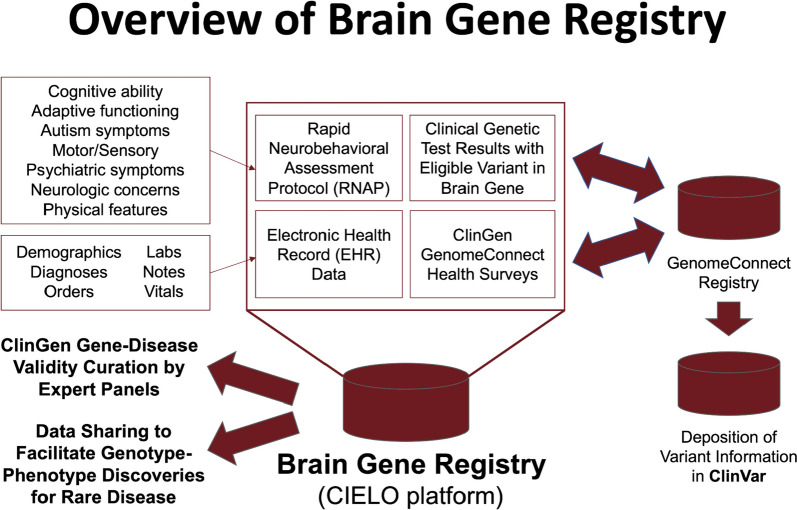
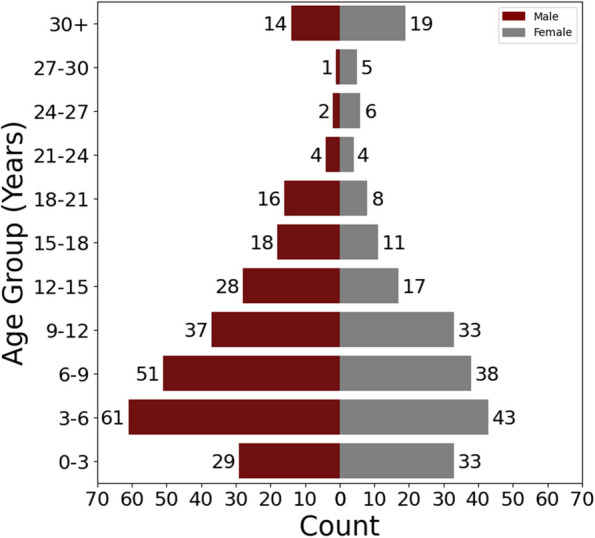
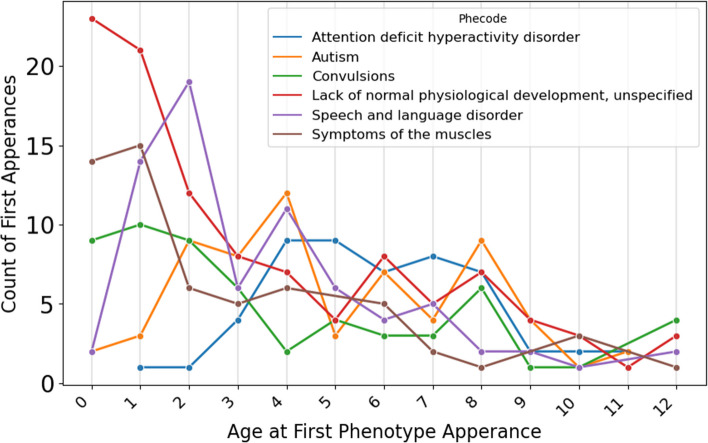
Monogenic disorders account for a large proportion of population-attributable risk for neurodevelopmental disabilities. However, the data necessary to infer a causal relationship between a given genetic variant and a particular neurodevelopmental disorder is often lacking. Recognizing this scientific roadblock, 13 Intellectual and Developmental Disabilities Research Centers (IDDRCs) formed a consortium to create the Brain Gene Registry (BGR), a repository pairing clinical genetic data with phenotypic data from participants with variants in putative brain genes. Phenotypic profiles are assembled from the electronic health record (EHR) and a battery of remotely administered standardized assessments collectively referred to as the Rapid Neurobehavioral Assessment Protocol (RNAP), which include cognitive, neurologic, and neuropsychiatric assessments, as well as assessments for attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). Co-enrollment of BGR participants in the Clinical Genome Resource's (ClinGen's) GenomeConnect enables display of variant information in ClinVar. The BGR currently contains data on 479 participants who are 55% male, 6% Asian, 6% Black or African American, 76% white, and 12% Hispanic/Latine. Over 200 genes are represented in the BGR, with 12 or more participants harboring variants in each of these genes: CACNA1A, DNMT3A, SLC6A1, SETD5, and MYT1L. More than 30% of variants are de novo and 43% are classified as variants of uncertain significance (VUSs). Mean standard scores on cognitive or developmental screens are below average for the BGR cohort. EHR data reveal developmental delay as the earliest and most common diagnosis in this sample, followed by speech and language disorders, ASD, and ADHD. BGR data has already been used to accelerate gene-disease validity curation of 36 genes evaluated by ClinGen's BGR Intellectual Disability (ID)-Autism (ASD) Gene Curation Expert Panel. In summary, the BGR is a resource for use by stakeholders interested in advancing translational research for brain genes and continues to recruit participants with clinically reported variants to establish a rich and well-characterized national resource to promote research on neurodevelopmental disorders.
Keywords: Brain gene registry; Electronic health records; Neurodevelopmental disorders.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures









References
-
- Association AP. Diagnostic and statistical manual of mental disorders : DSM-5. 5. Arlington, VA: American Psychiatric Association; 2013.
-
- Srivastava S, Love-Nichols JA, Dies KA, Ledbetter DH, Martin CL, Chung WK, et al. Meta-analysis and multidisciplinary consensus statement: exome sequencing is a first-tier clinical diagnostic test for individuals with neurodevelopmental disorders. Genet Med. 2019;21(11):2413–2421. doi: 10.1038/s41436-019-0554-6. - DOI - PMC - PubMed
-
- Manickam K, McClain MR, Demmer LA, Biswas S, Kearney HM, Malinowski J, et al. Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: an evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG) Genet Med. 2021;23(11):2029–2037. doi: 10.1038/s41436-021-01242-6. - DOI - PubMed
