

Complement propagates visual system pathology following traumatic brain injury
- PMID: 38632569
- PMCID: PMC11022420
- DOI: 10.1186/s12974-024-03098-4
Complement propagates visual system pathology following traumatic brain injury
Abstract
Background: Traumatic brain injury (TBI) is associated with the development of visual system disorders. Visual deficits can present with delay and worsen over time, and may be associated with an ongoing neuroinflammatory response that is known to occur after TBI. Complement system activation is strongly associated with the neuroinflammatory response after TBI, but whether it contributes to vision loss after TBI is unexplored.
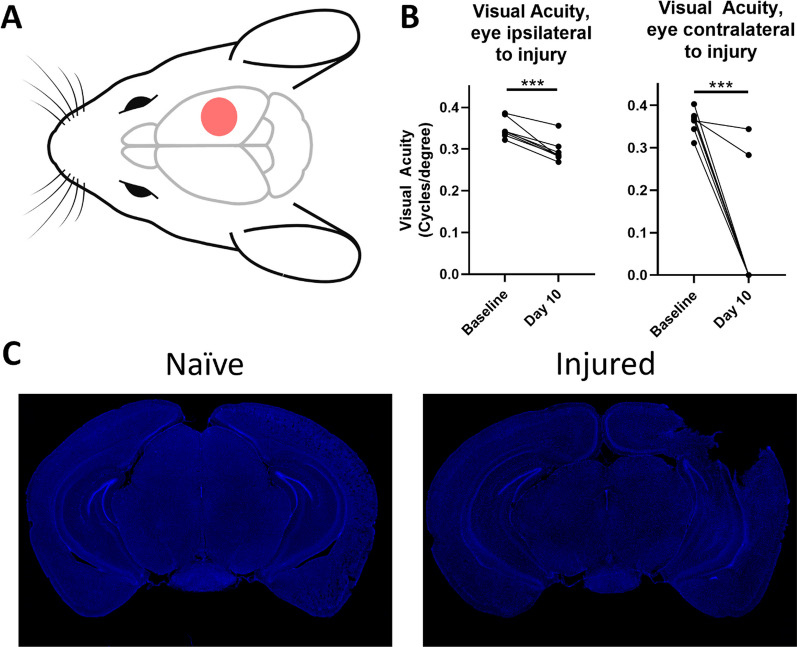
Methods: Acute and chronic neuroinflammatory changes within the dorsal lateral geniculate nucleus (dLGN) and retina were investigated subsequent to a moderate to severe murine unilateral controlled cortical impact. Neuroinflammatory and histopathological outcomes were interpreted in the context of behavioral and visual function data. To investigate the role of complement, cohorts were treated after TBI with the complement inhibitor, CR2-Crry.
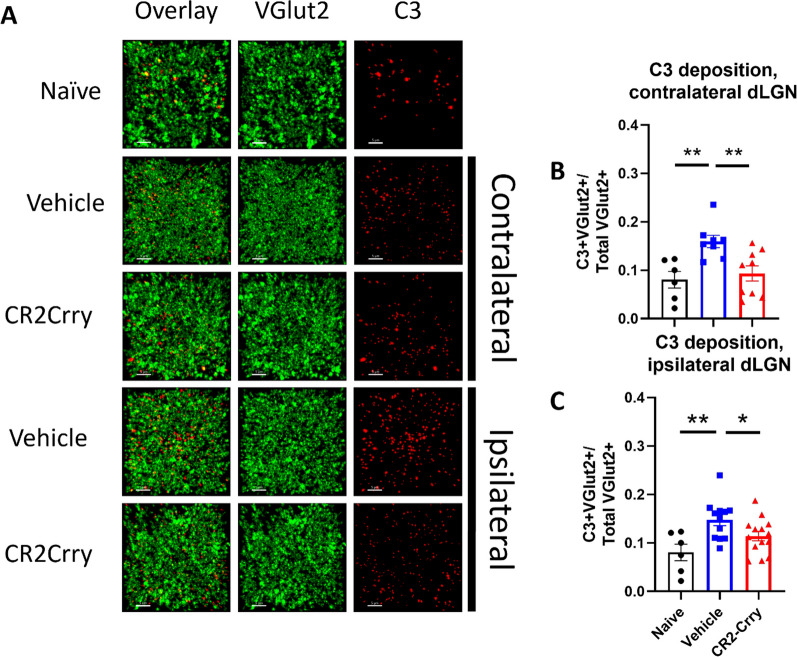
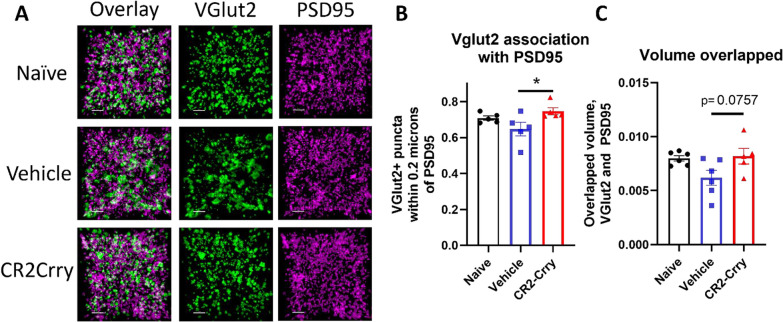
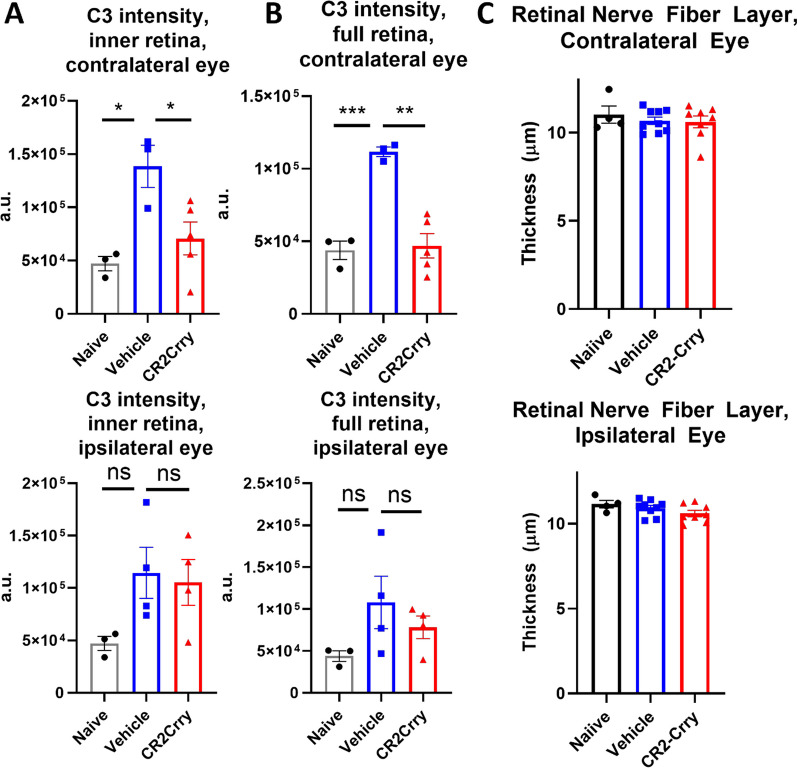
Results: At 3 days after TBI, complement component C3 was deposited on retinogeniculate synapses in the dLGN both ipsilateral and contralateral to the lesion, which was reduced in CR2-Crry treated animals. This was associated with microglia morphological changes in both the ipsilateral and contralateral dLGN, with a less ramified phenotype in vehicle compared to CR2-Crry treated animals. Microglia in vehicle treated animals also had a greater internalized VGlut2 + synaptic volume after TBI compared to CR2-Crry treated animals. Microglia morphological changes seen acutely persisted for at least 49 days after injury. Complement inhibition also reduced microglial synaptic internalization in the contralateral dLGN and increased the association between VGLUT2 and PSD95 puncta, indicating preservation of intact synapses. Unexpectedly, there were no changes in the thickness of the inner retina, retinal nerve fiber layer or retinal ganglion layer. Neuropathological changes in the dLGN were accompanied by reduced visual acuity at subacute and chronic time points after TBI, with improvement seen in CR2-Crry treated animals.
Conclusion: TBI induces complement activation within the dLGN and promotes microglial activation and synaptic internalization. Complement inhibition after TBI in a clinically relevant paradigm reduces complement activation, maintains a more surveillance-like microglia phenotype, and preserves synaptic density within the dLGN. Together, the data indicate that complement plays a key role in the development of visual deficits after TBI via complement-dependent microglial phagocytosis of synapses within the dLGN.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures





Update of
-
Complement propagates visual system pathology following traumatic brain injury.Res Sq [Preprint]. 2024 Feb 23:rs.3.rs-3970621. doi: 10.21203/rs.3.rs-3970621/v1. Res Sq. 2024. Update in: J Neuroinflammation. 2024 Apr 17;21(1):98. doi: 10.1186/s12974-024-03098-4. PMID: 38464312 Free PMC article. Updated. Preprint.
References
-
- Fulkerson DH, White IK, Rees JM, Baumanis MM, Smith JL, Ackerman LL, et al. Analysis of long-term (median 10.5 years) outcomes in children presenting with traumatic brain injury and an initial Glasgow Coma Scale score of 3 or 4. J Neurosurg Pediatrics PED. 2015;16(4):410–419. doi: 10.3171/2015.3.PEDS14679. - DOI - PubMed
-
- Goodrich GL, Flyg HM, Kirby JE, Chang C-Y, Martinsen GL. Mechanisms of TBI and visual consequences in military and veteran populations. Optometry Vision Sci. 2013;90(2). - PubMed
MeSH terms
Substances
Grants and funding
- I01 BX003050/BX/BLRD VA/United States
- I01 BX004256/BX/BLRD VA/United States
- R01EY030072/NH/NIH HHS/United States
- I01 RX000444/RX/RRD VA/United States
- P30 CA138313/CA/NCI NIH HHS/United States
- P20GM148302/NH/NIH HHS/United States
- I21 BX005853/BX/BLRD VA/United States
- IK6 BX005235/BX/BLRD VA/United States
- I01 RX003958/RX/RRD VA/United States
- R01 EY030072/EY/NEI NIH HHS/United States
- P20 GM148302/GM/NIGMS NIH HHS/United States
- IK6 BX004858/BX/BLRD VA/United States
- P30CA138313/NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
