

Effect of preoperative immunonutrition on postoperative short-term clinical outcomes in patients with gastric cancer cachexia: a prospective randomized controlled trial
- PMID: 38632641
- PMCID: PMC11022452
- DOI: 10.1186/s12957-024-03348-y
Effect of preoperative immunonutrition on postoperative short-term clinical outcomes in patients with gastric cancer cachexia: a prospective randomized controlled trial
Abstract
Background: Although current guidelines(ESPEN guideline: Clinical nutrition in surgery and other guidelines) recommend preoperative immunonutrition for cachectic gastric cancer patients, the strength of the recommendation is weak, and the level of evidence is low. The benefits of preoperative immunonutrition still remain controversial.
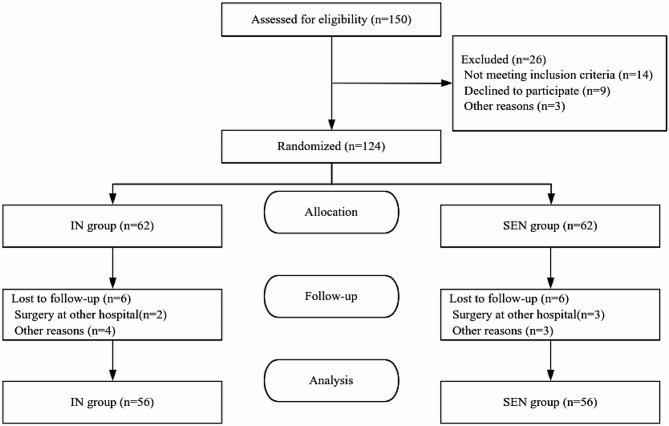
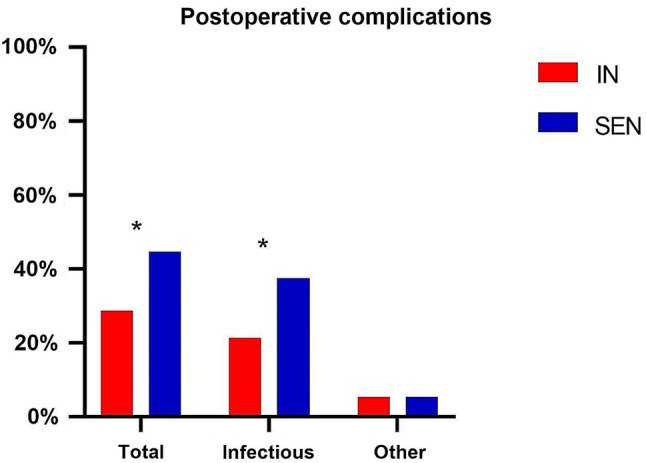
Patients and methods: 112 patients with gastric cancer cachexia were enrolled in the study and randomly assigned in a 1:1 ratio to receive either preoperative enteral immunonutrition support (IN, n = 56) or standard enteral nutrition support (SEN, n = 56). The primary endpoint was the incidence of infectious complications, and the secondary endpoints included the nutritional indicators, inflammatory markers, immune parameters, postoperative recovery and complications and gastrointestinal intolerance reactions.
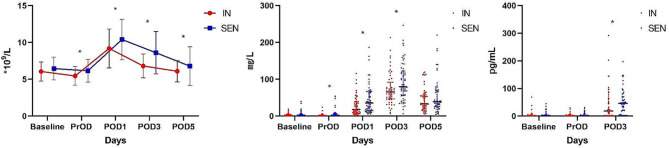
Results: The incidence of postoperative infectious complications(P = 0.040) and overall complications (P = 0.049)was significantly lower in the IN group compared to the SEN group. In terms of laboratory inflammatory indexes, patients in the IN group demonstrated significantly lower levels of white blood cells (WBC), C-reactive protein (CRP), and interleukin-6 (IL-6), as well as higher levels of lymphocytes (LYMPH) and immunoglobulin A (IgA), compared to patients in the SEN group, with statistically significant differences. In terms of clinical outcomes, the IN group had a shorter duration of antibiotic use (P = 0.048), shorter hospital stay (P = 0.018), and lower total hospital costs (P = 0.034) compared to the SEN group. The IN group also experienced significantly less weight loss after surgery (P = 0.043).
Conclusion: Preoperative administration of immunonutrition formula has a positive impact on the incidence of infectious complications in patients with gastric cancer cachexia after surgery. It improves patients' inflammatory and immune status, shortens hospital stays, and reduces healthcare costs. Preoperative use of immunonutrition may contribute to the improvement of prognosis in this high-risk population.
Keywords: Cancer cachexia; Enteral nutrition; Gastric cancer; Immunonutrition; Preoperative intervention.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
