

Incorporation, adaptation and rejection of obstetric practices during the implementation of the "Adequate Childbirth Program" in Brazilian private hospitals: a qualitative study
- PMID: 38632645
- PMCID: PMC11022312
- DOI: 10.1186/s12978-024-01772-7
Incorporation, adaptation and rejection of obstetric practices during the implementation of the "Adequate Childbirth Program" in Brazilian private hospitals: a qualitative study
Abstract
Background: The "Adequate Childbirth Program" (PPA) is a quality improvement project that aims to reduce the high rates of unnecessary cesarean section in Brazilian private hospitals. This study aimed to analyze labor and childbirth care practices after the first phase of PPA implementation.
Method: This study uses a qualitative approach. Eight hospitals were selected. At each hospital, during the period of 5 (five) days, from July to October 2017, the research team conducted face to face interviews with doctors (n = 21) and nurses (n = 28), using semi-structured scripts. For the selection of professionals, the Snowball technique was used. The interviews were transcribed, and the data submitted to Thematic Content Analysis, using the MaxQda software.
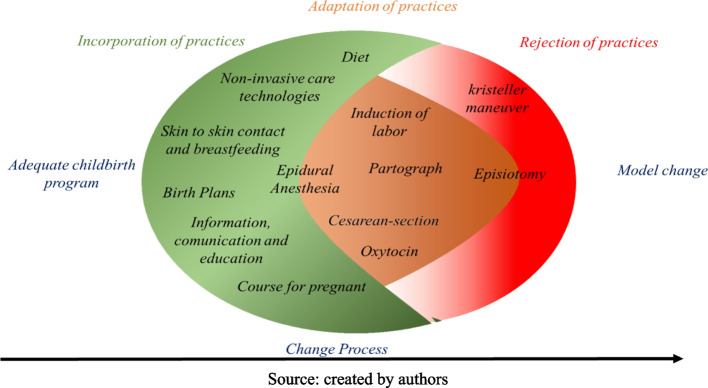
Results: The three analytical dimensions of the process of change in the care model: (1) Incorporation of care practices: understood as the practices that have been included since PPA implementation; (2) Adaptation of care practices: understood as practices carried out prior to PPA implementation, but which underwent modifications with the implementation of the project; (3) Rejection of care practices: understood as those practices that were abandoned or questioned whether or not they should be carried out by hospital professionals.
Conclusions: After the PPA, changes were made in hospitals and in the way, women were treated. Birth planning, prenatal hospital visits led by experts (for expecting mothers and their families), diet during labor, pharmacological analgesia for vaginal delivery, skin-to-skin contact, and breastfeeding in the first hour of life are all included. To better monitor labor and vaginal birth and to reduce CS without a clinical justification, hospitals adjusted their present practices. Finally, the professionals rejected the Kristeller maneuver since research has demonstrated that using it's harmful.
Keywords: Health evaluation; Healthcare models; Hospitals; Midwifery; Obstetrics; Private; Quality improvement.
Plain language summary
Brazil has high Cesarean Section (CS) rates, with rates far from the ideal recommended by the World Health Organization and a model of care that does not favor women’s autonomy and empowerment. In 2015, a quality improvement project, called “Projeto Parto Adequado” (PPA), was implemented in Brazilian private hospitals to reduce unnecessary cesarean section, in addition to encouraging the process of natural and safe childbirth. One of the components of this project was to reorganize the model of care in hospitals to prepare professionals for humanized and safe care. The data were collected in 8 hospitals with interviews with 49 professionals, approximately two years after the beginning of the project in the hospitals. There were changes in the hospital routine and in the care of women after the project. The professionals incorporated practices such as skin-to-skin contact and breastfeeding; diet during labor; non-invasive care technologies, especially to relieve pain during labor; birth plan; pregnancy courses with guided tours in hospitals (for pregnant women and family); and analgesia for vaginal labor. There was adaptation of existing practices in hospitals to reduce CS that had no clinical indication; better monitoring of labor, favoring vaginal delivery. And finally, the professionals rejected the practice that presses the uterine fundus, for not having shown efficacy in recent studies. We can conclude that the hospitals that participated in this study have made an effort to change their obstetric model. However, specific aspects of each hospital, the organization of the health system in Brazil, and the incentive of the local administration influenced the implementation of these changes by professionals in practice.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Evaluation of labor and childbirth care by nurse-midwives in Brazilian private hospitals: results of a quality improvement project.Reprod Health. 2023 Jan 19;20(Suppl 2):17. doi: 10.1186/s12978-022-01537-0. Reprod Health. 2023. PMID: 36658552 Free PMC article.
-
Process of adhesion of the Adequate Childbirth Program to improve obstetric care in private hospitals in Brazil.Reprod Health. 2023 Jan 6;20(Suppl 2):9. doi: 10.1186/s12978-022-01542-3. Reprod Health. 2023. PMID: 36609380 Free PMC article.
-
Women's voice on changes in childbirth care practices: a qualitative approach to women's experiences in Brazilian private hospitals participating in the Adequate Childbirth Project.Reprod Health. 2023 Jan 24;20(Suppl 2):19. doi: 10.1186/s12978-022-01539-y. Reprod Health. 2023. PMID: 36694218 Free PMC article.
-
Women's autonomy in the process of labour and childbirth: integrative literature review.Rev Gaucha Enferm. 2017 Apr 20;38(1):e64677. doi: 10.1590/1983-1447.2017.01.64677. Rev Gaucha Enferm. 2017. PMID: 28443976 English, Portuguese.
-
[Continuous support during childbirth to reduce cesarean sections: evidence brief for policy].Cien Saude Colet. 2022 Feb;27(2):427-439. doi: 10.1590/1413-81232022272.41572020. Epub 2020 Dec 19. Cien Saude Colet. 2022. PMID: 35137801 Review. Portuguese.
Cited by
-
Achievements and Challenges in the Development of a Nurse-Led Respectful Delivery Care Model Provided by Partners in Health in Rural Mexico.Public Health Nurs. 2025 Jan-Feb;42(1):435-443. doi: 10.1111/phn.13443. Epub 2024 Oct 23. Public Health Nurs. 2025. PMID: 39439405 Free PMC article.
-
The effects of a quality improvement project to reduce caesarean sections in selected private hospitals in Brazil.Reprod Health. 2024 Sep 4;20(Suppl 2):194. doi: 10.1186/s12978-024-01851-9. Reprod Health. 2024. PMID: 39232837 Free PMC article.
References
-
- ANS AN de SS. Histórico - Linha do tempo. Available at: http://www.ans.gov.br/aans/quem-somos/historico. Citado 13 de fevereiro de 2021.
-
- Appropriate technology for birth. Lancet. 1985;2(8452):436–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
