

An early-onset specific polygenic risk score optimizes age-based risk estimate and stratification of prostate cancer: population-based cohort study
- PMID: 38632662
- PMCID: PMC11025178
- DOI: 10.1186/s12967-024-05190-y
An early-onset specific polygenic risk score optimizes age-based risk estimate and stratification of prostate cancer: population-based cohort study
Abstract
Background: Early-onset prostate cancer (EOPC, ≤ 55 years) has a unique clinical entity harboring high genetic risk, but the majority of EOPC patients still substantial opportunity to be early-detected thus suffering an unfavorable prognosis. A refined understanding of age-based polygenic risk score (PRS) for prostate cancer (PCa) would be essential for personalized risk stratification.
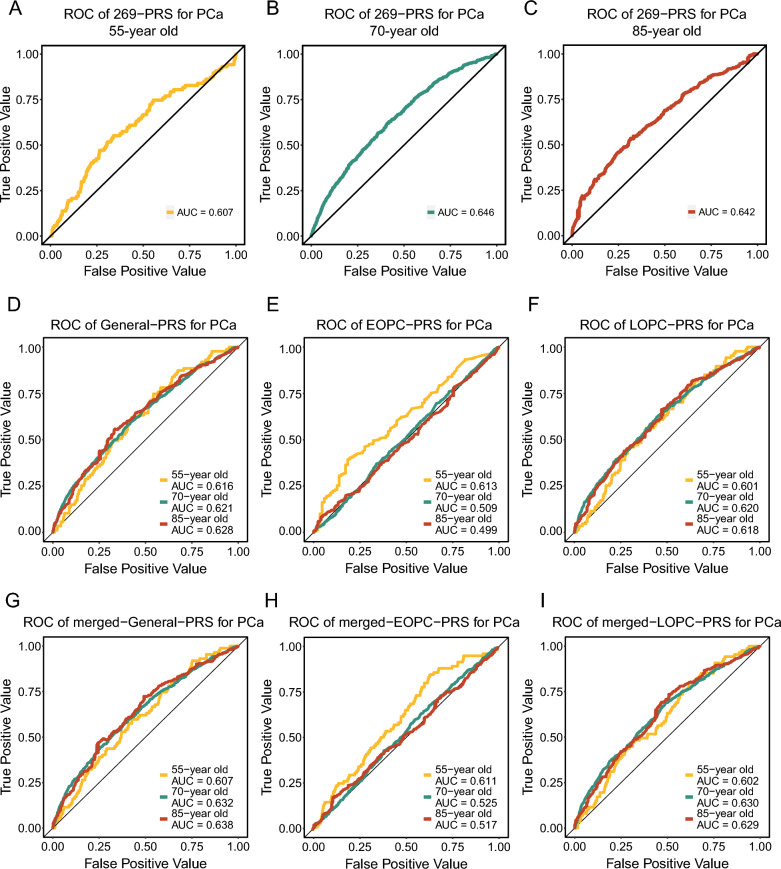
Methods: We included 167,517 male participants [4882 cases including 205 EOPC and 4677 late-onset PCa (LOPC)] from UK Biobank. A General-, an EOPC- and an LOPC-PRS were derived from age-specific genome-wide association studies. Weighted Cox proportional hazard models were applied to estimate the risk of PCa associated with PRSs. The discriminatory capability of PRSs were validated using time-dependent receiver operating characteristic (ROC) curves with additional 4238 males from PLCO and TCGA. Phenome-wide association studies underlying Mendelian Randomization were conducted to discover EOPC linking phenotypes.
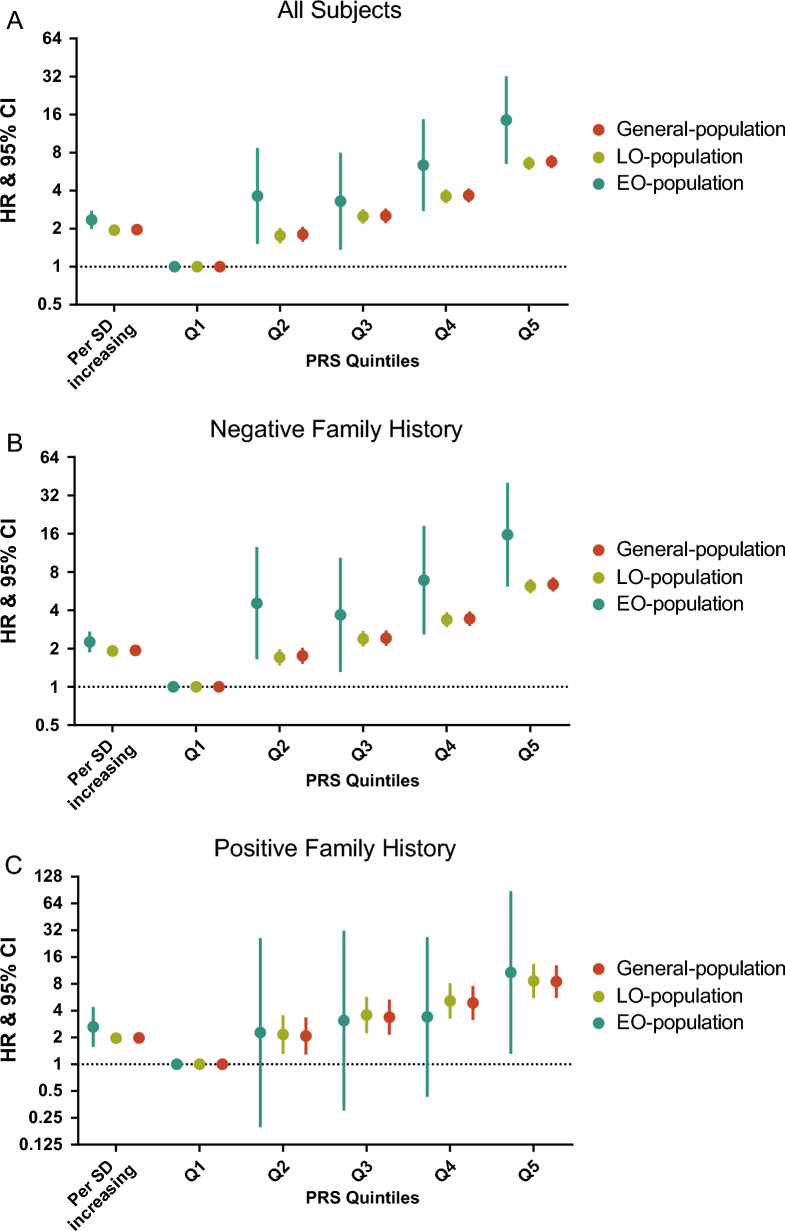
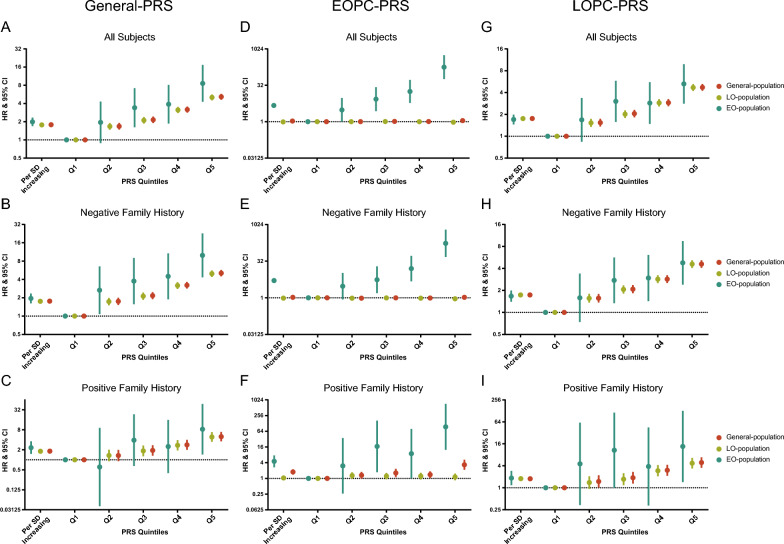
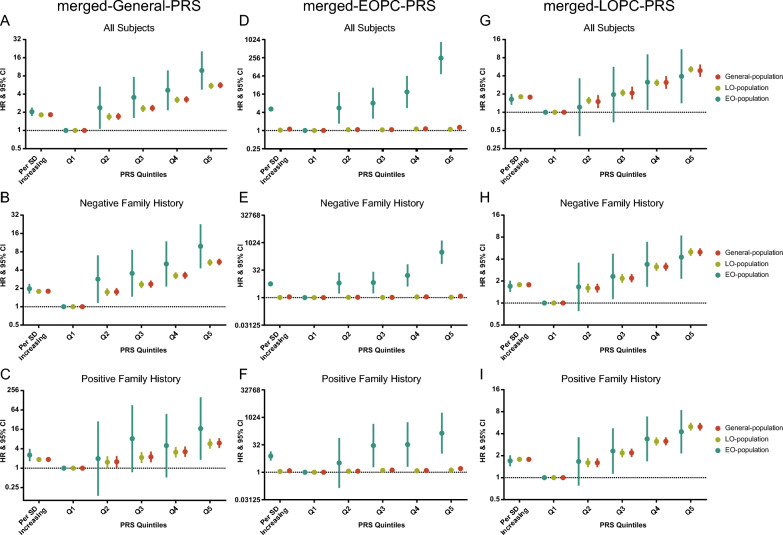
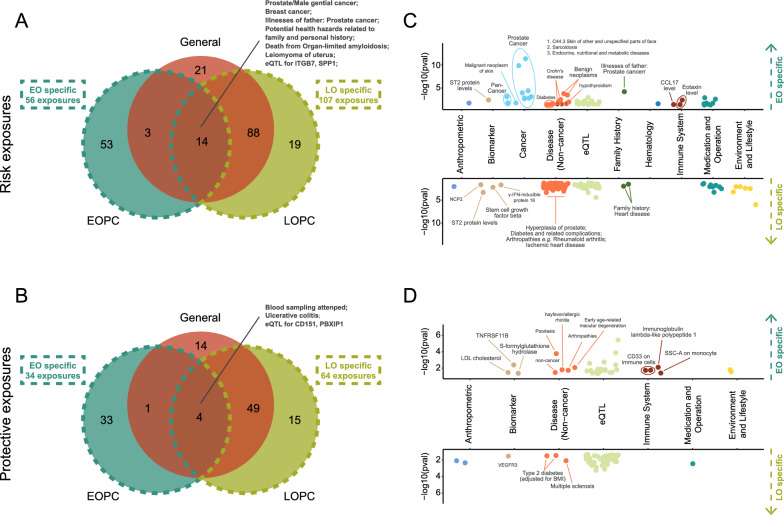
Results: The 269-PRS calculated via well-established risk variants was more strongly associated with risk of EOPC [hazard ratio (HR) = 2.35, 95% confidence interval (CI) 1.99-2.78] than LOPC (HR = 1.95, 95% CI 1.89-2.01; I2 = 79%). EOPC-PRS was dramatically related to EOPC risk (HR = 4.70, 95% CI 3.98-5.54) but not to LOPC (HR = 0.98, 95% CI 0.96-1.01), while LOPC-PRS had similar risk estimates for EOPC and LOPC (I2 = 0%). Particularly, EOPC-PRS performed optimal discriminatory capability for EOPC (area under the ROC = 0.613). Among the phenomic factors to PCa deposited in the platform of ProAP (Prostate cancer Age-based PheWAS; https://mulongdu.shinyapps.io/proap ), EOPC was preferentially associated with PCa family history while LOPC was prone to environmental and lifestyles exposures.
Conclusions: This study comprehensively profiled the distinct genetic and phenotypic architecture of EOPC. The EOPC-PRS may optimize risk estimate of PCa in young males, particularly those without family history, thus providing guidance for precision population stratification.
Keywords: Age-specific genome-wide association studies; Early-onset prostate cancer; Phenome-wide association studies; Polygenic risk score; UK biobank.
© 2024. The Author(s).
Conflict of interest statement
L.W. provided consulting service to Pupil Bio lnc. and reviewed manuscripts for
Figures
Similar articles
-
Early-onset pancreatic cancer: a population-based study using the SEER registry.Langenbecks Arch Surg. 2019 Aug;404(5):565-571. doi: 10.1007/s00423-019-01810-0. Epub 2019 Aug 3. Langenbecks Arch Surg. 2019. PMID: 31377855 Free PMC article.
-
Polygenic risk scores for the prediction of common cancers in East Asians: A population-based prospective cohort study.Elife. 2023 Mar 27;12:e82608. doi: 10.7554/eLife.82608. Elife. 2023. PMID: 36971353 Free PMC article.
-
Polygenic risk score-based phenome-wide association study of head and neck cancer across two large biobanks.BMC Med. 2024 Mar 14;22(1):120. doi: 10.1186/s12916-024-03305-2. BMC Med. 2024. PMID: 38486201 Free PMC article.
-
Early-onset pancreatic cancer: a review of molecular mechanisms, management, and survival.Oncotarget. 2022 Jun 15;13:828-841. doi: 10.18632/oncotarget.28242. eCollection 2022. Oncotarget. 2022. PMID: 35720978 Free PMC article. Review.
-
Early-onset pancreatic cancer: A national cancer registry study from the Czech Republic and review of the literature.J Hepatobiliary Pancreat Sci. 2023 Dec;30(12):1324-1333. doi: 10.1002/jhbp.1359. Epub 2023 Sep 26. J Hepatobiliary Pancreat Sci. 2023. PMID: 37750364 Review.
Cited by
-
Single-cell and spatial RNA sequencing identify divergent microenvironments and progression signatures in early- versus late-onset prostate cancer.Nat Aging. 2025 May;5(5):909-928. doi: 10.1038/s43587-025-00842-0. Epub 2025 Apr 10. Nat Aging. 2025. PMID: 40211000
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
