

Assessing multidisciplinary follow-up pattern efficiency and cost in follow-up care for patients in cervical spondylosis surgery: a non-randomized controlled study
- PMID: 38633312
- PMCID: PMC11022215
- DOI: 10.3389/fmed.2024.1354483
Assessing multidisciplinary follow-up pattern efficiency and cost in follow-up care for patients in cervical spondylosis surgery: a non-randomized controlled study
Abstract
Background: The use of multidisciplinary treatment programs in out-of-hospital healthcare is a new area of research. Little is known about the benefits of this method in the management of discharged patients undergoing cervical spondylosis surgery.
Objective: This study aimed to explore the effect of a contracted-based, multidisciplinary follow-up plan in patients after cervical spondylosis surgery.
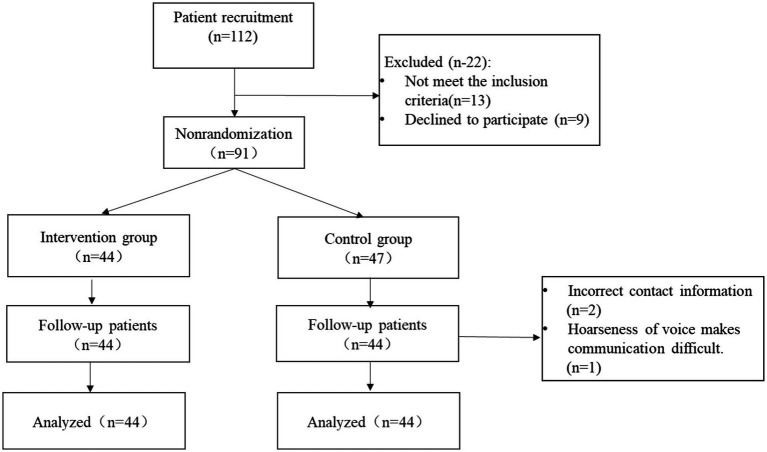
Methods: This non-blinded non-randomized controlled study was conducted with 88 patients (44 in the intervention group, 44 in the control group). The clinical outcomes, including Neck Disability Index (NDI), pain score (VAS), Self-Efficacy for Managing Chronic Disease 6-item Scale (SECD-6), and 12-Item Short-Form Health Survey (SF-12) score were assessed at the time of discharge, 24-72 h, 1 month, and 3 months post-discharge. The complications, patient satisfaction, and economic indicators were assessed at the final follow-up (3 months).
Results: Patients who received contracted follow-up showed greater improvement in neck dysfunction at 24-72 h, 1 month, and 3 months after discharge compared to those who received routine follow-up (p < 0.001). At 1 month after discharge, the intervention group exhibited better self-efficacy (p = 0.001) and quality of life (p < 0.001) than the control group, and these improvements lasted for 3 months. The intervention group reported lower pain scores at 24-72 h and 1 month (p = 0.008; p = 0.026) compared to the control group. The incidence of complications was significantly lower in the intervention group (11.4%) compared to the control group (40.9%). The total satisfaction score was significant difference between the two groups (p < 0.001). Additionally, the intervention group had lower direct medical costs (p < 0.001), direct non-medical costs (p = 0.035), and total costs (p = 0.04) compared to the control group. However, there was no statistically significant difference in indirect costs between the two groups (p = 0.59).
Conclusion: A multidisciplinary contract follow-up plan has significant advantages regarding neck disability, self-efficacy, quality of life, postoperative complications, patient satisfaction, and direct costs compared with routine follow-up.
Keywords: cervical spondylosis surgery; continuity of care; contracted follow-up pattern; cost; multidisciplinary team.
Copyright © 2024 Fu, Xie, Li, Gao, Chen and Ning.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Is depression the contraindication of anterior cervical decompression and fusion for cervical spondylosis?Front Endocrinol (Lausanne). 2022 Sep 30;13:1031616. doi: 10.3389/fendo.2022.1031616. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36246923 Free PMC article.
-
Cost-Effectiveness of Jingshu Granules Compared to Placebo for the Treatment of Patients with Cervical Radiculopathy in China: A Decision-Tree Model Based on Randomized Controlled Trial.J Altern Complement Med. 2019 Dec;25(12):1183-1192. doi: 10.1089/acm.2019.0262. Epub 2019 Oct 30. J Altern Complement Med. 2019. PMID: 31634001 Clinical Trial.
-
Artificial discs for lumbar and cervical degenerative disc disease -update: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(10):1-98. Epub 2006 Apr 1. Ont Health Technol Assess Ser. 2006. PMID: 23074480 Free PMC article.
-
Comparison of the short- and long-term treatment effect of cervical disk replacement and anterior cervical disk fusion: a meta-analysis.Eur J Orthop Surg Traumatol. 2015 Jul;25 Suppl 1:S87-100. doi: 10.1007/s00590-014-1469-1. Epub 2014 May 5. Eur J Orthop Surg Traumatol. 2015. PMID: 24791930 Review.
-
Clinical efficacy and safety of posterior minimally invasive surgery in cervical spondylosis: a systematic review.J Orthop Surg Res. 2022 Aug 13;17(1):389. doi: 10.1186/s13018-022-03274-3. J Orthop Surg Res. 2022. PMID: 35964065 Free PMC article.
References
-
- Kang S. A full strategy for the rescue of cervical spondylosis. Changchun, China: Jilin Science and Technology Press; (2008).
-
- Davies BM, Phillips R, Clarke D, Furlan JC, Demetriades AK, Milligan J, et al. . Establishing the socio-economic impact of degenerative cervical myelopathy is fundamental to improving outcomes [AO spine RECODE-DCM research priority number 8]. Glob Spine J. (2022) 12:122S–9S. doi: 10.1177/21925682211039835 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources