

FAPi PET/CT for assessment and visualisation of active myositis-related interstitial lung disease: a prospective observational pilot study
- PMID: 38633577
- PMCID: PMC11019096
- DOI: 10.1016/j.eclinm.2024.102598
FAPi PET/CT for assessment and visualisation of active myositis-related interstitial lung disease: a prospective observational pilot study
Abstract
Background: Interstitial lung disease (ILD) is a common manifestation of idiopathic inflammatory myopathies (IIM) and a substantial contributor to hospitalisation, increased morbidity, and mortality. In-vivo evidence of ongoing tissue remodelling in IIM-ILD is scarce. We aimed to evaluate fibroblast activation in lungs of IIM-patients and control individuals using ⁶⁸Ga-labelled inhibitor of Fibroblast-Activation-Protein (FAPi) based positronic emission tomography and computed tomography imaging (PET/CT).
Methods: In this prospective observational pilot study, consecutive patients with IIM and participants without rheumatic conditions or ILD serving as a control group were recruited at the Medical University of Vienna, Austria, and underwent FAPi PET/CT imaging. Standard-of-care procedures including clinical examination, assessment of severity of dyspnoea, high-resolution computed tomography (HR-CT), and pulmonary function testing (PFT) were performed on all patients with IIM at baseline and for patients with IIM-ILD at follow-up of 12 months. Baseline pulmonary FAPi-uptake was assessed by the maximum (SUVmax) and mean (SUVmean) standardized uptake values (SUV) over the whole lung (wl). SUV was corrected for blood pool background activity and target-to-background ratios (TBR) were calculated. We compared pulmonary FAPi-uptake between patients with IIM-ILD and those without ILD, as well as controls, and correlated baseline FAP-uptake with standard diagnostic tools such as HR-CT and PFT. For predictive implications, we investigated whether patients with IIM and progressive ILD exhibited higher baseline FAPi-uptake compared to those with stable ILD. Metrics are reported as mean with standard deviation (±SD).
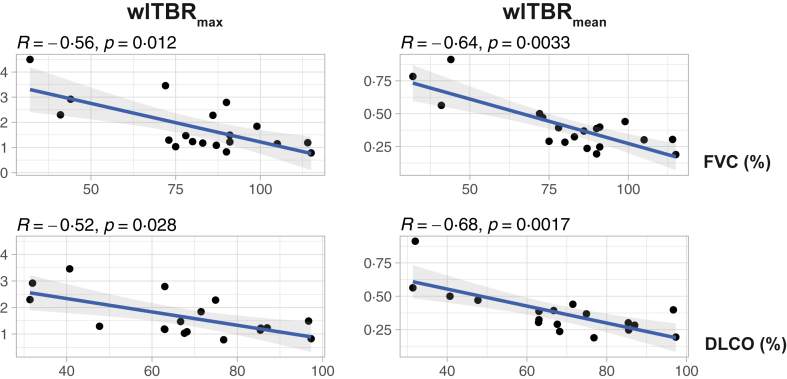
Findings: Between November 16, 2021 and October 10, 2022, a total of 32 patients were enrolled in the study. Three participants from the control group were excluded due to cardiopulmonary disease. In individuals with IIM-ILD (n = 14), wlTBRmax and wlTBRmean were significantly increased as compared with both non-ILD-IIM patients (n = 5) and the control group (n = 16): wlTBRmax: 2.06 ± 1.04 vs. 1.04 ± 0.22 (p = 0.019) and 1.08 ± 0.19 (p = 0.0012) and wlTBRmean: 0.45 ± 0.19 vs. 0.26 ± 0.06 (p = 0.025) and 0.27 ± 0.07 (p = 0.0024). Similar values were observed in wlTBRmax or wlTBRmean between non-ILD IIM patients and the control group. Patients with progressive ILD displayed significantly enhanced wlTBRmax and wlTBRmean values at baseline compared to patients with stable ILD: wlTBRmax: 1.30 ± 0.31 vs. 2.63 ± 1.04 (p = 0.0084) and wlTBRmean: 0.32 ± 0.08 vs. 0.55 ± 0.19 (p = 0.021). Strong correlations were found between FAPi-uptake and disease extent on HR-CT (wlTBRmax: R = 0.42, p = 0.07; wlTBRmean: R = 0.56, p = 0.013) and severity of respiratory symptoms determined by the New York Heart Association (NYHA) classification tool (wlTBRmax: R = 0.52, p = 0.022; wlTBRmean: R = 0.59, p = 0.0073). Further, pulmonary FAPi-uptake showed inverse correlation with forced vital capacity (FVC) (wlTBRmax: R = -0.56, p = 0.012; wlTBRmean: R = -0.64, p = 0.0033) and diffusing capacity of the lungs for carbon monoxide (DLCO) (wlTBRmax: R = -0.52, p = 0.028; wlTBRmean: R = -0.68, p = 0.0017).
Interpretation: Our study demonstrates higher fibroblast activation in patients with IIM-ILD compared to non-ILD patients and controls. Intensity of pulmonary FAPi accumulation was associated with progression of ILD. Considering that this study was carried out on a small population, FAPi PET/CT may serve as a useful non-invasive tool for risk stratification of lung disease in IIM.
Funding: The Austrian Research Fund.
Keywords: Fibroblast activation; Fibrosis; Idiopathic inflammatory myopathy; Interstitial lung disease.
© 2024 The Authors.
Conflict of interest statement
KK reports honoraria for lectures and presentations from UCB Pharma, Boehringer Ingelheim, Eli Lilly and AbbVie; support for attending meetings and/or travel: AbbVie, AstraZeneca and Bristol-Myers Squibb. ES reports support for attending meetings and/or travel from Pfizer, Bristol-Myers Squibb, Boehringer-Ingelheim and AstraZeneca. DM reports honoraria from AstraZeneca and travel support from Pfizer. MB received grants from GSK. HP received grants from Siemens, Boehringer-Ingelheim and AstraZeneca; reported honoraria for lectures and presentations from Boehringer-Ingelheim, AstraZeneca and Roche, and participation on a data safety monitoring board/advisory board for Siemens and Boehringer-Ingelheim. DA received grants, speaker fees, or consultancy fees from Abbvie, Gilead, Galapagos, Eli Lilly, Janssen, Merck, Novartis, Pfizer, Sandoz, and Sanofi. HR reports honoraria for lectures and presentations from Gilead, Merck and Pfizer; support for attending meetings and/or travel from Janssen. TSN, OCK, IG, HPK, FP, WL, TTW, SB, MH, and PM declare no competing interests.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous
