

Rapid Metabolism Underlying Subtherapeutic Serum Levels of Atypical Antipsychotics Preceding Clozapine Treatment: A Retrospective Analysis of Real-World Data
- PMID: 38635089
- PMCID: PMC11098931
- DOI: 10.1007/s40263-024-01079-y
Rapid Metabolism Underlying Subtherapeutic Serum Levels of Atypical Antipsychotics Preceding Clozapine Treatment: A Retrospective Analysis of Real-World Data
Abstract
Introduction: Adequate antipsychotic treatment intensity is required before diagnosing resistant schizophrenia and initiating clozapine treatment. We aimed to investigate potential rapid drug metabolism underlying low dose-adjusted serum concentration (CD) of non-clozapine atypical antipsychotics preceding clozapine treatment.
Methods: Patients using non-clozapine, atypical antipsychotics (aripiprazole, risperidone, olanzapine, or quetiapine) within 1 year before starting clozapine were included in this study from a therapeutic drug monitoring service in Oslo, Norway, between 2005 and 2023. Patients were assigned into low CD (LCD) and normal CD (NCD) subgroups. Using a reference sample with 147,964 antipsychotic measurements, LCD was defined as CDs below the 25th percentile, while patients with NCD exhibited CDs between the 25th and 75th percentile of the respective reference measurements. Metabolic ratios, doses, and frequency of subtherapeutic levels of non-clozapine antipsychotics were compared between LCD and NCD groups.
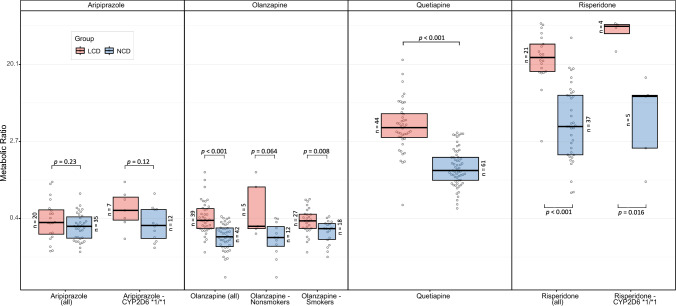
Results: Preceding clozapine treatment, 110 out of 272 included patients (40.4%) were identified with LCD. Compared with the NCD group, LCD patients exhibited higher metabolic ratios of olanzapine (1.5-fold; p < 0.001), quetiapine (3.0-fold; p < 0.001), and risperidone (6.0-fold; p < 0.001). Metabolic ratio differences were independent of smoking and CYP2D6 genotype for olanzapine (p = 0.008) and risperidone (p = 0.016), respectively. Despite higher doses of olanzapine (1.25-fold; p = 0.054) and quetiapine (1.6-fold; p = 0.001) in LCD versus NCD patients, faster metabolism among the former was accompanied by higher frequencies of subtherapeutic levels of olanzapine (3.3-fold; p = 0.044) and quetiapine (1.8-fold; p = 0.005).
Conclusion: LCD and associated rapid metabolism of non-clozapine antipsychotics is frequent before starting clozapine treatment. For olanzapine and quetiapine, this is associated with significantly increased risk of having subtherapeutic concentrations.
© 2024. The Author(s).
Conflict of interest statement
OAA is consultant to Cortechs.ai and received speaker’s honoraria from Lundbeck, Sunovion, Janssen. The other authors have no competing interests to declare that are relevant to the content of this article.
Figures
References
-
- Howes OD, McCutcheon R, Agid O, de Bartolomeis A, van Beveren NJM, Birnbaum ML, et al. Treatment resistant schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) working group consensus guidelines on diagnosis and terminology. Am J Psychiatry. 2017;174:216–229. doi: 10.1176/appi.ajp.2016.16050503. - DOI - PMC - PubMed
-
- Huhn M, Nikolakopoulou A, Schneider-Thoma J, Krause M, Samara M, Peter N, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394:939–951. doi: 10.1016/S0140-6736(19)31135-3. - DOI - PMC - PubMed
-
- Miller DD. Review and management of clozapine side effects. J Clin Psychiatry. 2000;61(Suppl 8):14–17. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
