

Biomarker Predictors of Clinical Efficacy of the Anti-IgE Biologic Omalizumab in Severe Asthma in Adults: Results of the SoMOSA Study
- PMID: 38635834
- PMCID: PMC11348961
- DOI: 10.1164/rccm.202310-1730OC
Biomarker Predictors of Clinical Efficacy of the Anti-IgE Biologic Omalizumab in Severe Asthma in Adults: Results of the SoMOSA Study
Abstract
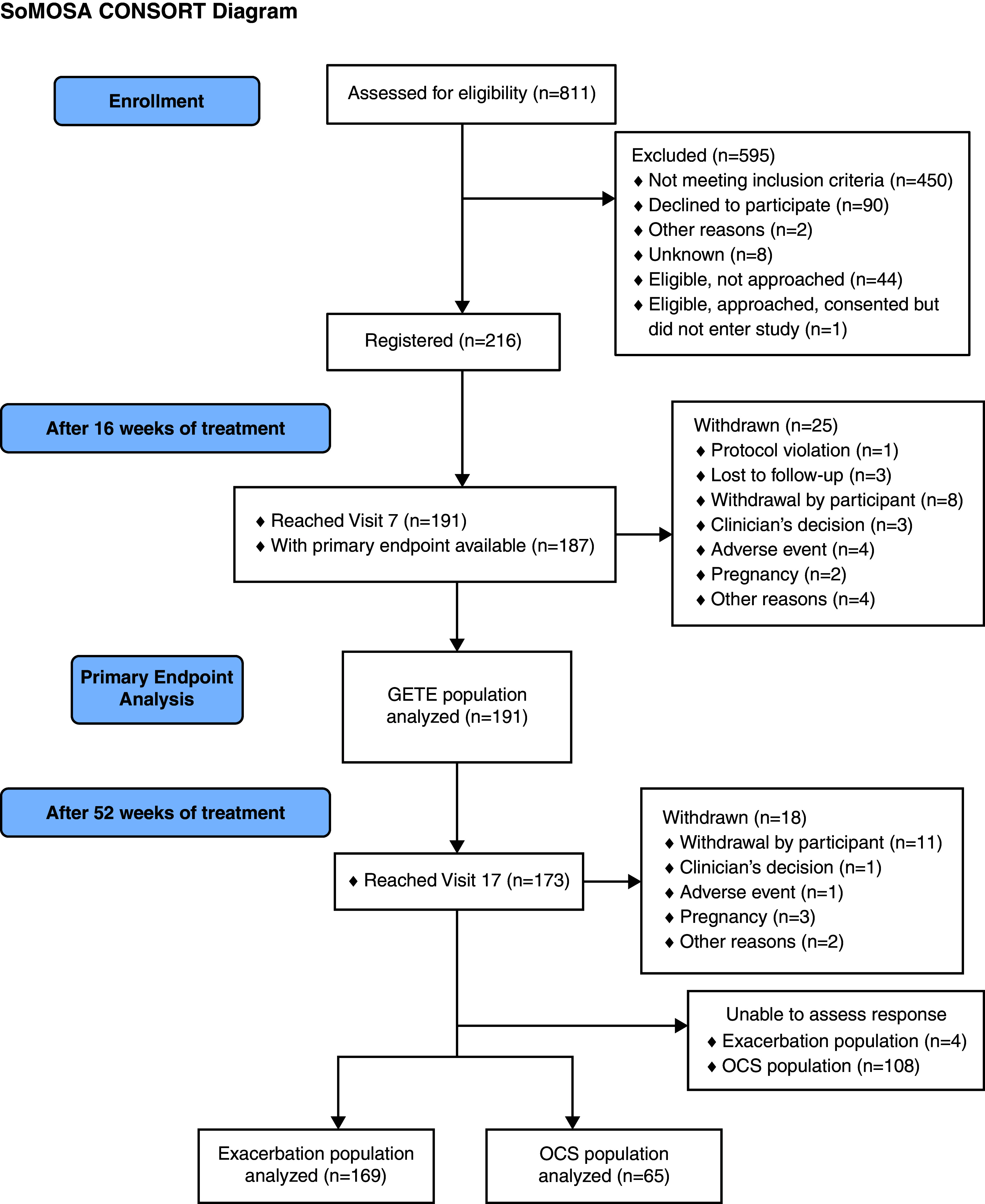
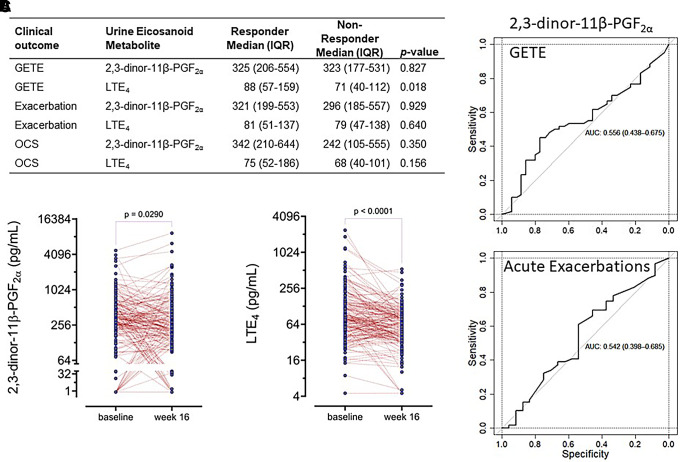
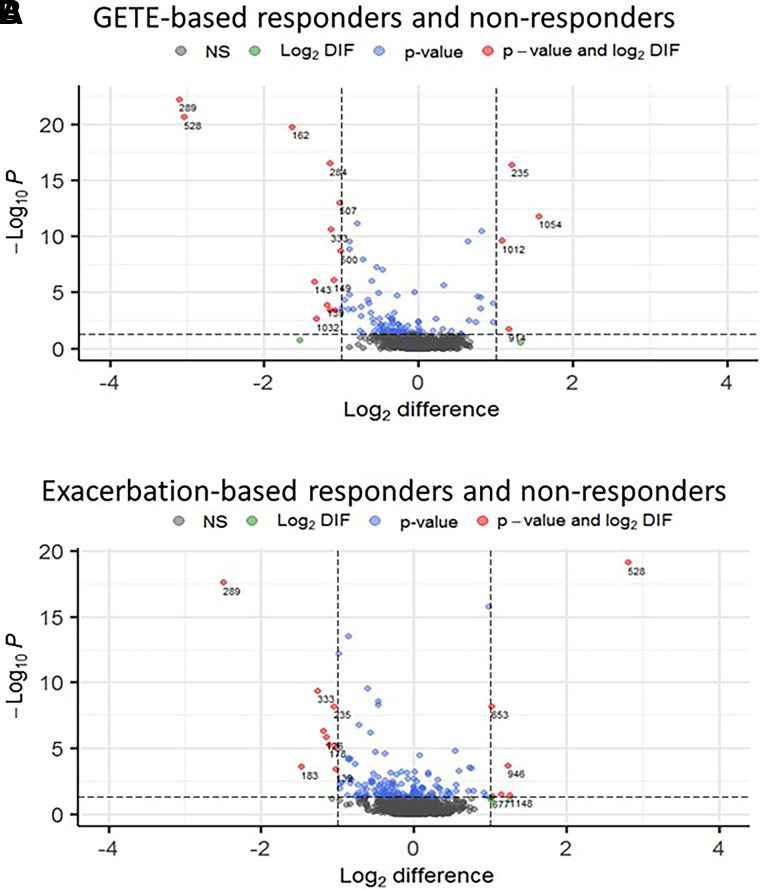
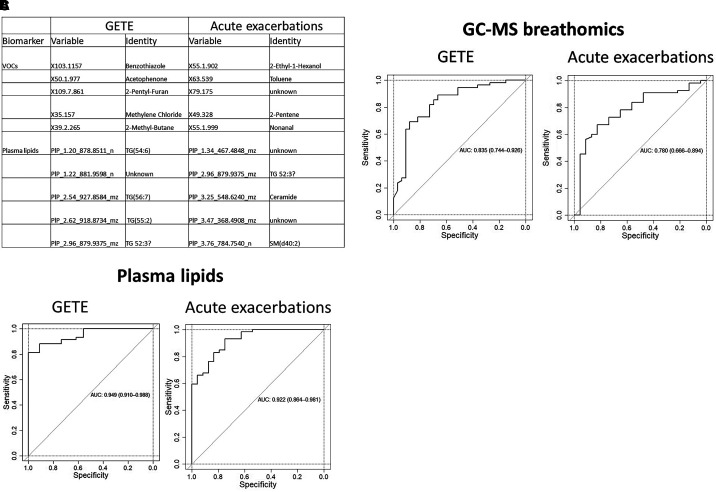
Background: The anti-IgE monoclonal antibody omalizumab is widely used for severe asthma. This study aimed to identify biomarkers that predict clinical improvement during 1 year of omalizumab treatment. Methods: One-year open-label Study of Mechanisms of action of Omalizumab in Severe Asthma (SoMOSA) involving 216 patients with severe (Global Initiative for Asthma step 4/5) uncontrolled atopic asthma (at least two severe exacerbations in the previous year) taking high-dose inhaled corticosteroids and long-acting β-agonists with or without maintenance oral corticosteroids. It had two phases: 0-16 weeks, to assess early clinical improvement by Global Evaluation of Therapeutic Effectiveness (GETE); and 16-52 weeks, to assess late responses based on ⩾50% reduction in exacerbations or mOCS dose. All participants provided samples (exhaled breath, blood, sputum, urine) before and after 16 weeks of omalizumab treatment. Measurements and Main Results: A total of 191 patients completed phase 1; 63% had early improvement. Of 173 who completed phase 2, 69% had reduced exacerbations by ⩾50% and 57% (37 of 65) taking mOCSs had reduced their dose by ⩾50%. The primary outcomes 2,3-dinor-11-β-PGF2α, GETE score, and standard clinical biomarkers (blood and sputum eosinophils, exhaled nitric oxide, serum IgE) did not predict either clinical response. Five volatile organic compounds and five plasma lipid biomarkers strongly predicted the ⩾50% reduction in exacerbations (receiver operating characteristic areas under the curve of 0.780 and 0.922, respectively) and early responses (areas under the curve of 0.835 and 0.949, respectively). In an independent cohort, gas chromatography/mass spectrometry biomarkers differentiated between severe and mild asthma. Conclusions: This is the first discovery of omics biomarkers that predict improvement in asthma with biologic agent treatment. Prospective validation and development for clinical use is justified.
Figures
Comment in
-
Strategies for Identifying Biomarkers in Severe Asthma.Am J Respir Crit Care Med. 2024 Aug 1;210(3):251-252. doi: 10.1164/rccm.202404-0707ED. Am J Respir Crit Care Med. 2024. PMID: 38701409 Free PMC article. No abstract available.
References
-
- Hanania NA, Alpan O, Hamilos DL, Condemi JJ, Reyes-Rivera I, Zhu J, et al. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann Intern Med . 2011;154:573–582. - PubMed
-
- Hanania NA, Wenzel S, Rosén K, Hsieh HJ, Mosesova S, Choy DF, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med . 2013;187:804–811. - PubMed
-
- Bousquet J, Cabrera P, Berkman N, Buhl R, Holgate S, Wenzel S, et al. The effect of treatment with omalizumab, an anti-IgE antibody, on asthma exacerbations and emergency medical visits in patients with severe persistent asthma. Allergy . 2005;60:302–308. - PubMed
-
- Bousquet J, Rabe K, Humbert M, Chung KF, Berger W, Fox H, et al. Predicting and evaluating response to omalizumab in patients with severe allergic asthma. Respir Med . 2007;101:1483–1492. - PubMed
-
- Kroes JA, Zielhuis SW, van Roon EN, Ten Brinke A. Prediction of response to biological treatment with monoclonal antibodies in severe asthma. Biochem Pharmacol . 2020;179:113978. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
