

Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021
- PMID: 38636536
- PMCID: PMC11339187
- DOI: 10.1016/S1473-3099(24)00176-2
Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021
Abstract
Background: Lower respiratory infections (LRIs) are a major global contributor to morbidity and mortality. In 2020-21, non-pharmaceutical interventions associated with the COVID-19 pandemic reduced not only the transmission of SARS-CoV-2, but also the transmission of other LRI pathogens. Tracking LRI incidence and mortality, as well as the pathogens responsible, can guide health-system responses and funding priorities to reduce future burden. We present estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 of the burden of non-COVID-19 LRIs and corresponding aetiologies from 1990 to 2021, inclusive of pandemic effects on the incidence and mortality of select respiratory viruses, globally, regionally, and for 204 countries and territories.
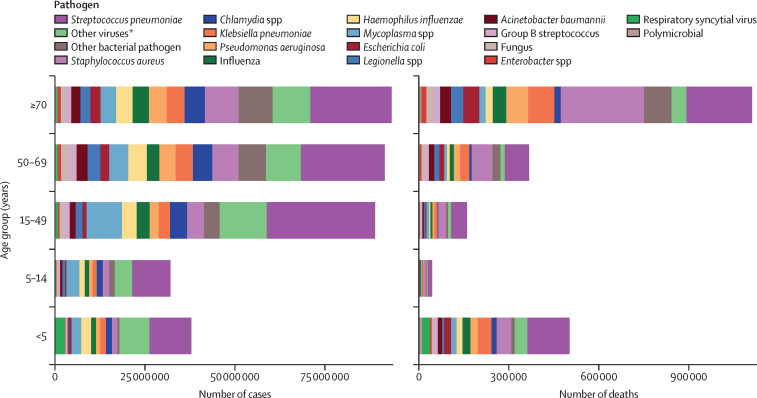
Methods: We estimated mortality, incidence, and aetiology attribution for LRI, defined by the GBD as pneumonia or bronchiolitis, not inclusive of COVID-19. We analysed 26 259 site-years of mortality data using the Cause of Death Ensemble model to estimate LRI mortality rates. We analysed all available age-specific and sex-specific data sources, including published literature identified by a systematic review, as well as household surveys, hospital admissions, health insurance claims, and LRI mortality estimates, to generate internally consistent estimates of incidence and prevalence using DisMod-MR 2.1. For aetiology estimation, we analysed multiple causes of death, vital registration, hospital discharge, microbial laboratory, and literature data using a network analysis model to produce the proportion of LRI deaths and episodes attributable to the following pathogens: Acinetobacter baumannii, Chlamydia spp, Enterobacter spp, Escherichia coli, fungi, group B streptococcus, Haemophilus influenzae, influenza viruses, Klebsiella pneumoniae, Legionella spp, Mycoplasma spp, polymicrobial infections, Pseudomonas aeruginosa, respiratory syncytial virus (RSV), Staphylococcus aureus, Streptococcus pneumoniae, and other viruses (ie, the aggregate of all viruses studied except influenza and RSV), as well as a residual category of other bacterial pathogens.
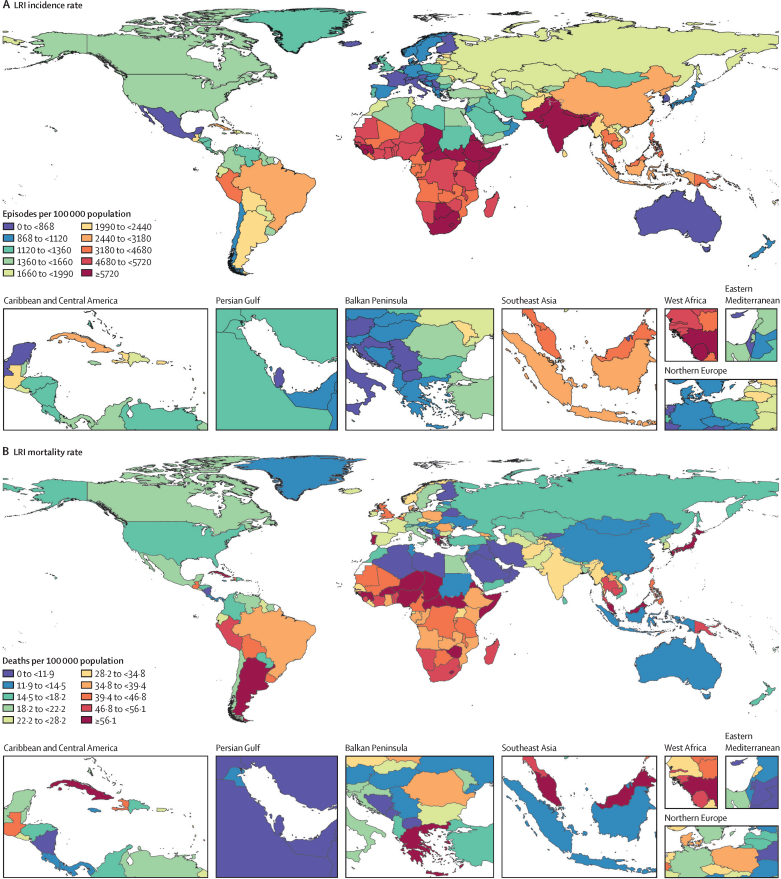
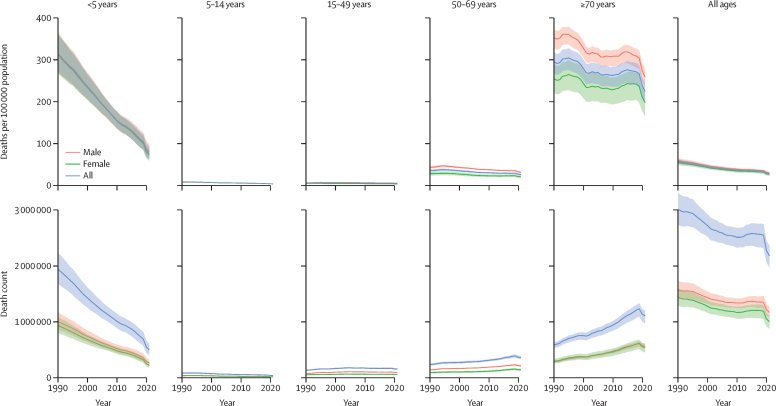
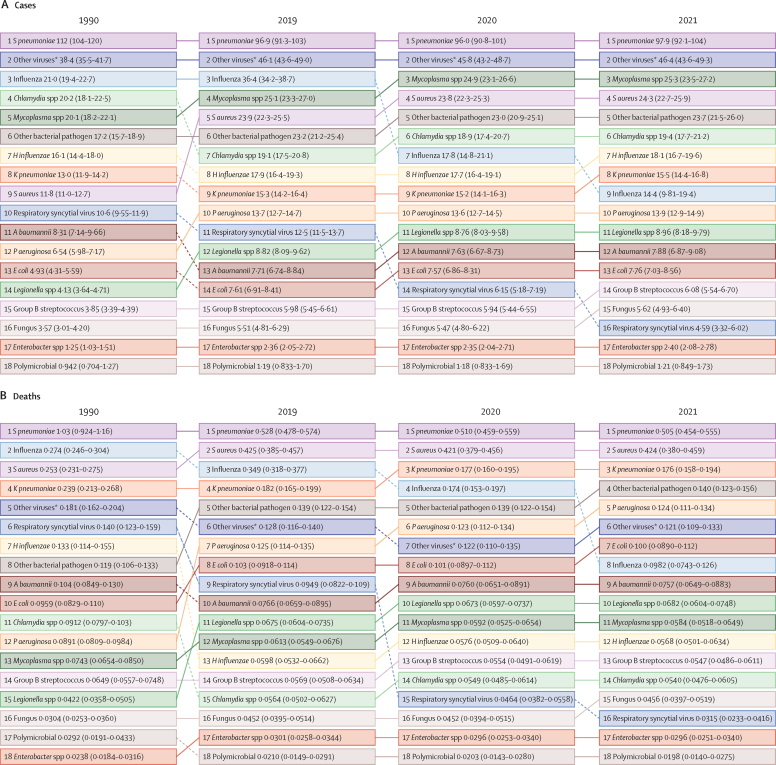
Findings: Globally, in 2021, we estimated 344 million (95% uncertainty interval [UI] 325-364) incident episodes of LRI, or 4350 episodes (4120-4610) per 100 000 population, and 2·18 million deaths (1·98-2·36), or 27·7 deaths (25·1-29·9) per 100 000. 502 000 deaths (406 000-611 000) were in children younger than 5 years, among which 254 000 deaths (197 000-320 000) occurred in countries with a low Socio-demographic Index. Of the 18 modelled pathogen categories in 2021, S pneumoniae was responsible for the highest proportions of LRI episodes and deaths, with an estimated 97·9 million (92·1-104·0) episodes and 505 000 deaths (454 000-555 000) globally. The pathogens responsible for the second and third highest episode counts globally were other viral aetiologies (46·4 million [43·6-49·3] episodes) and Mycoplasma spp (25·3 million [23·5-27·2]), while those responsible for the second and third highest death counts were S aureus (424 000 [380 000-459 000]) and K pneumoniae (176 000 [158 000-194 000]). From 1990 to 2019, the global all-age non-COVID-19 LRI mortality rate declined by 41·7% (35·9-46·9), from 56·5 deaths (51·3-61·9) to 32·9 deaths (29·9-35·4) per 100 000. From 2019 to 2021, during the COVID-19 pandemic and implementation of associated non-pharmaceutical interventions, we estimated a 16·0% (13·1-18·6) decline in the global all-age non-COVID-19 LRI mortality rate, largely accounted for by a 71·8% (63·8-78·9) decline in the number of influenza deaths and a 66·7% (56·6-75·3) decline in the number of RSV deaths.
Interpretation: Substantial progress has been made in reducing LRI mortality, but the burden remains high, especially in low-income and middle-income countries. During the COVID-19 pandemic, with its associated non-pharmaceutical interventions, global incident LRI cases and mortality attributable to influenza and RSV declined substantially. Expanding access to health-care services and vaccines, including S pneumoniae, H influenzae type B, and novel RSV vaccines, along with new low-cost interventions against S aureus, could mitigate the LRI burden and prevent transmission of LRI-causing pathogens.
Funding: Bill & Melinda Gates Foundation, Wellcome Trust, and Department of Health and Social Care (UK).
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests J A Berkley reports support for the present manuscript from research grants from the Bill & Melinda Gates Foundation, Wellcome Trust, the National Institute for Health and Care Research (NIHR), and the Medical Research Council (MRC). C Brown reports other financial support from an ad-hoc one-off market research advisory role (anonymously conducted via market research companies with no direct communication, none specifically related to lower respiratory tract infections), all outside the submitted work. K Krishan reports other non-financial support from the UGC Centre of Advanced Study, CAS II, awarded to the Department of Anthropology, Panjab University (Chandigarh, India) outside the submitted work. M-C Li reports support for the present manuscript from the National Science and Technology Council in Taiwan (112-2410-H-003-031) and other financial or non-financial support as a Technical Editor of the Journal of the American Heart Association, Review Editor of Frontiers in Public Health, and Editorial Board Member of BMC Public Health, outside the submitted work. S A Meo reports grants or contracts from King Saud University (Riyadh, Saudi Arabia; RSP-2024 R47), outside the submitted work. L Monasta reports support for the present manuscript from the Italian Ministry of Health (Ricerca Corrente 34/2017), with payments made to the Institute for Maternal and Child Health IRCCS Burlo Garofolo. C Moore reports participation with Dr Gwen Knight as a member of the advisory board for MRC grants (no payments made), with the WHO Advisory group, and with the REVIVE Advisory group as a member of the steering group; and leadership or fiduciary roles in board, society, committee, or advocacy groups (unpaid) as the co-chair of the Impact and Influence Group of the Microbiology Society, outside the submitted work. A Pollard reports grants or contracts from the Bill & Melinda Gates Foundation, Wellcome Trust, Cepi, MRC, NIHR, AstraZeneca, European Commission, and the Serum Institute of India; royalties or licenses from AstraZeneca; consulting fees from Shionogi; leadership or fiduciary roles in board, society, committee, or advocacy groups (unpaid) as the chair of the Department of Health and Social Care's Joint Committee on Vaccination and Immunisation and as a member of the WHO Strategic Advisory Group of Experts on Immunization until 2022; and receipt of equipment, materials, drugs, medical writing, gifts, or other services from Moderna, outside the submitted work. L F Reyes reports grants or contracts from MSD and Pfizer; consulting fees from GlaxoSmithKline, MSD, and Pfizer; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from GlaxoSmithKline, MSD, and Pfizer; payment for expert testimony from GlaxoSmithKline, MSD, and Pfizer; and support for attending meetings or travel from GlaxoSmithKline and Pfizer, outside the submitted work. Y L Samodra reports grants or contracts from Taipei Medical University, and leadership or fiduciary roles in board, society, committee, or advocacy groups (paid or unpaid) as the co-founder of Benang Merah Research Center, outside the submitted work. E A F Simôes reports support for the present manuscript from the Bill & Melinda Gates Foundation; grants or contracts from AstraZeneca, Merck & Co, Pfizer, and Icosavax; consulting fees from Merck & Co, Pfizer, GlaxoSmithKline, Sanofi Pasteur, Cidara Therapeutics, Adagio Therapeutics, Nuance Pharmaceuticals, Enanta, and Icosavax; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Pfizer and AstraZeneca; support for attending meetings or travel from Pfizer and AstraZeneca; and participation on a data safety monitoring board or advisory board with AbbVie, GlaxoSmithKline, the Bill & Melinda Gates Foundation, and Moderna, outside the submitted work. M Zielińska reports other financial support as an AstraZeneca employee, outside the submitted work.
Figures
References
-
- WHO Global health estimates. https://www.who.int/data/global-health-estimates
-
- Falagas ME, Mourtzoukou EG, Vardakas KZ. Sex differences in the incidence and severity of respiratory tract infections. Respir Med. 2007;101:1845–1863. - PubMed
-
- Ursin RL, Klein SL. Sex differences in respiratory viral pathogenesis and treatments. Annu Rev Virol. 2021;8:393–414. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
