

Transseptal coronary artery-a pictorial review
- PMID: 38637337
- PMCID: PMC11255081
- DOI: 10.1007/s00247-024-05911-x
Transseptal coronary artery-a pictorial review
Abstract
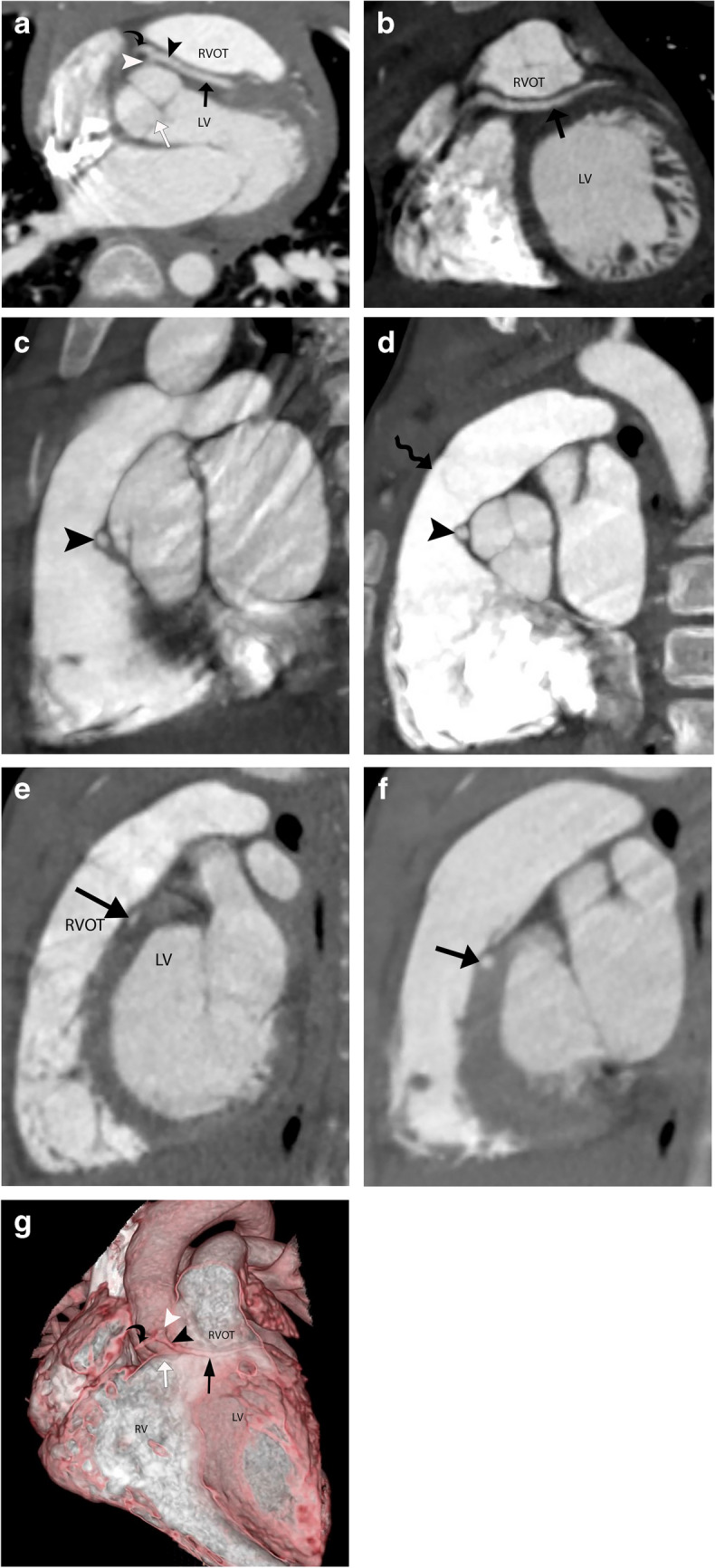
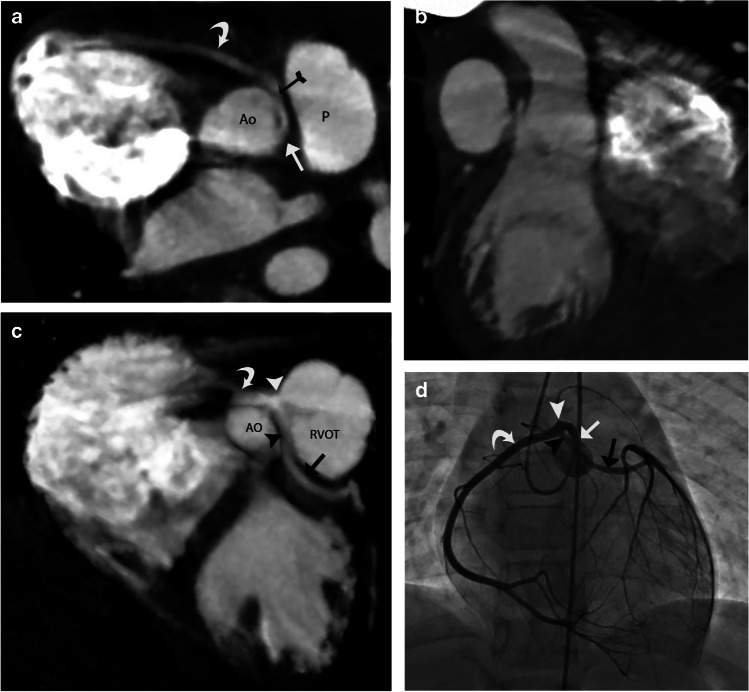
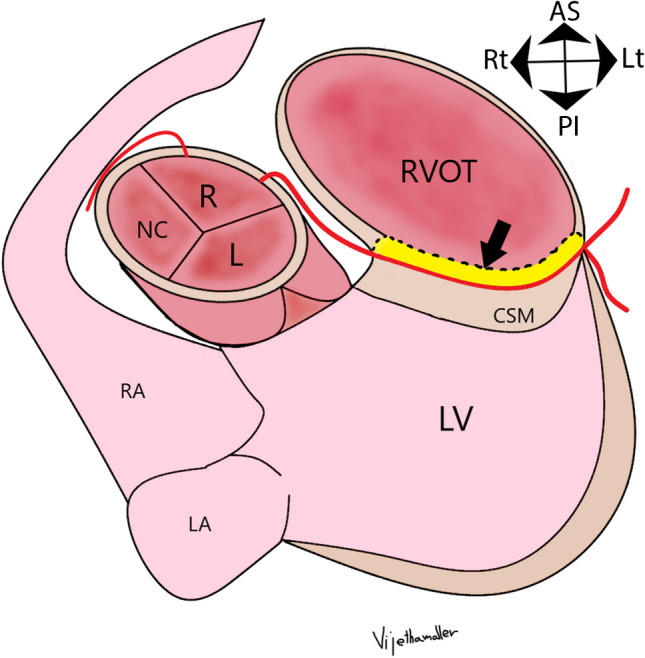
A transseptal coronary artery course, also known as a transconal course, is an anomalous course of the left main coronary artery (LMCA) or the left anterior descending artery (LAD) through the conal septal myocardium. The conal septal myocardium is the posterior wall of the right ventricular outflow tract (RVOT), acting as a dividing myocardial wall between the subaortic and subpulmonary outflow tracts. The initial segment of a transseptal coronary artery has an extraconal course between the aorta and the RVOT cranial to the true intramyocardial segment. The transseptal coronary artery then emerges out of the conal septal myocardium at the epicardial surface on the lateral aspect of the RVOT. Many consider the transseptal coronary artery to be a benign entity. However, there are few case reports of severe cardiac symptoms such as myocardial ischemia, arrhythmia, and even sudden cardiac deaths due to potential coronary artery compression in the systolic phase. In this article, we seek to describe the imaging findings of transseptal coronary artery course on coronary computed tomography angiography (CTA), discuss their clinical analysis, and briefly discuss the management of these lesions.
Keywords: Coronary artery; Interarterial; Intramural; Transconal; Transseptal; Unroofing; Virtual endoluminal.
© 2024. The Author(s).
Conflict of interest statement
None
Figures


References
-
- Molossi S, Agrawal H, Mery CM, Krishnamurthy R, Masand P, Sexson Tejtel SK, Noel CV, Qureshi AM, Jadhav SP, McKenzie ED, Fraser CD Jr (2020) Outcomes in anomalous aortic origin of a coronary artery following a prospective standardized approach. Circ Cardiovasc Interv 13 - PubMed
-
- Brothers JA, Whitehead KK, Keller MS, Fogel MA, Paridon SM, Weinberg PM, Harris MA. Cardiac MRI and CT: differentiation of normal ostium and intraseptal course from slitlike ostium and interarterial course in anomalous left coronary artery in children. AJR Am J Roentgenol. 2015;204:W104–109. doi: 10.2214/AJR.14.12953. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
