

Polytherapy versus monotherapy in the treatment of tibial non-unions: a retrospective study
- PMID: 38637406
- PMCID: PMC11026327
- DOI: 10.1186/s10195-024-00763-5
Polytherapy versus monotherapy in the treatment of tibial non-unions: a retrospective study
Abstract
Background: Treating tibial non-unions efficiently presents a challenge for orthopaedic trauma surgeons. The established gold standard involves implanting autologous bone graft with adequate fixation, but the addition of biologicals according to the so-called diamond concept has become increasingly popular in the treatment of non-unions. Previous studies have indicated that polytherapy, which involves implanting mesenchymal stem cells, bioactive factors and osteoconductive scaffolds, can improve bone healing. This study aims to evaluate the efficacy of polytherapy compared with monotherapy in treating tibial non-unions of varying severity.
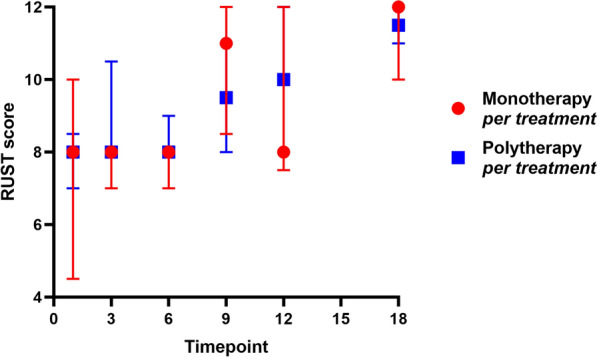
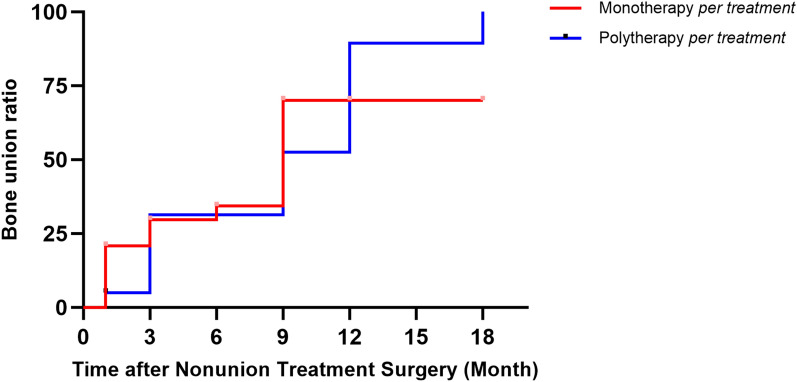
Materials and methods: Data from consecutive tibial non-unions treated between November 2014 and July 2023 were retrospectively analysed. The Non Union Scoring System (NUSS) score before non-union surgery, and the Radiographic Union Score for Tibial fractures (RUST), scored at 1, 3, 6, 9, 12 and 18 months post-surgery, were recorded. Initially, a comparison was made between the polytherapy and monotherapy groups. Subsequently, patients receiving additional surgical non-union treatment were documented, and the frequency of these treatments was tallied for a subsequent per-treatment analysis.
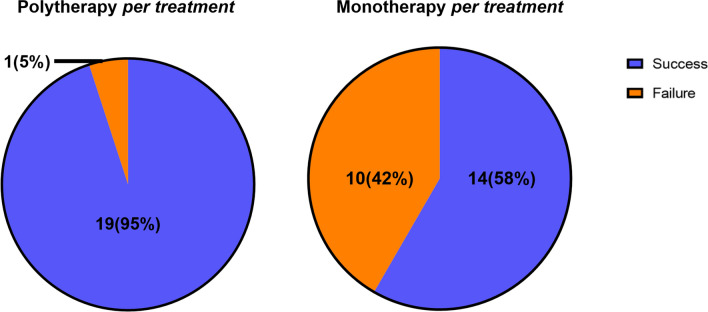
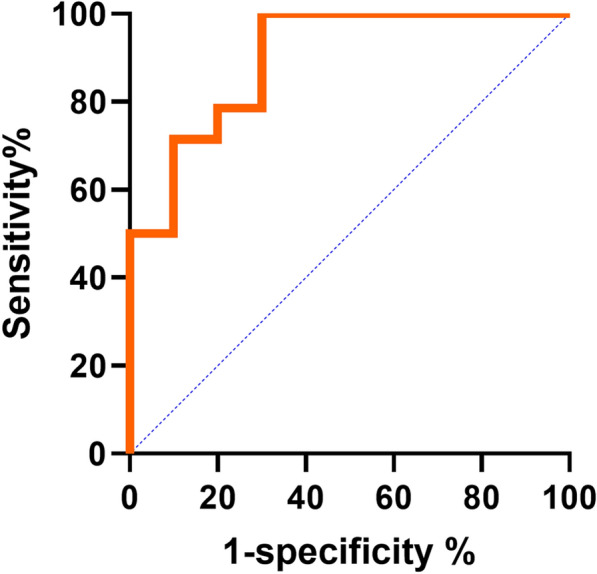
Results: A total of 34 patients were included and divided into a polytherapy group (n = 15) and a monotherapy group (n = 19). The polytherapy group demonstrated a higher NUSS score (44 (39, 52) versus 32 (29, 43), P = 0.019, z = -2.347) and a tendency towards a higher success rate (93% versus 68%, P = 0.104) compared with the monotherapy group. For the per-treatment analysis, 44 treatments were divided into the polytherapy per-treatment group (n = 20) and the monotherapy per-treatment group (n = 24). The polytherapy per-treatment group exhibited a higher NUSS score (48 (43, 60) versus 38 (30, 50), P = 0.030, z = -2.173) and a higher success rate (95% versus 58%, P = 0.006) than the monotherapy per-treatment group. Within the monotherapy per-treatment group, the NUSS score displayed excellent predictive performance (AUC = 0.9143). Setting the threshold value at 48, the sensitivity and specificity were 100.0% and 70.0%, respectively.
Conclusions: Polytherapy is more effective than monotherapy for severe tibial non-unions, offering a higher success ratio. The NUSS score supports decision-making in treating tibial non-unions.
Level of evidence: Level III.
Keywords: Monotherapy; NUSS; Polytherapy; RUST; Tibial non-union.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
