

Tumor-infiltrating lymphocytes in HER2-positive breast cancer treated with neoadjuvant chemotherapy and dual HER2-blockade
- PMID: 38637568
- PMCID: PMC11026378
- DOI: 10.1038/s41523-024-00636-4
Tumor-infiltrating lymphocytes in HER2-positive breast cancer treated with neoadjuvant chemotherapy and dual HER2-blockade
Abstract
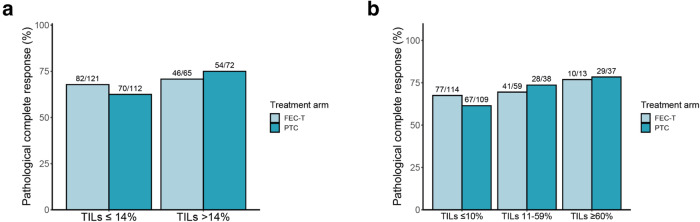
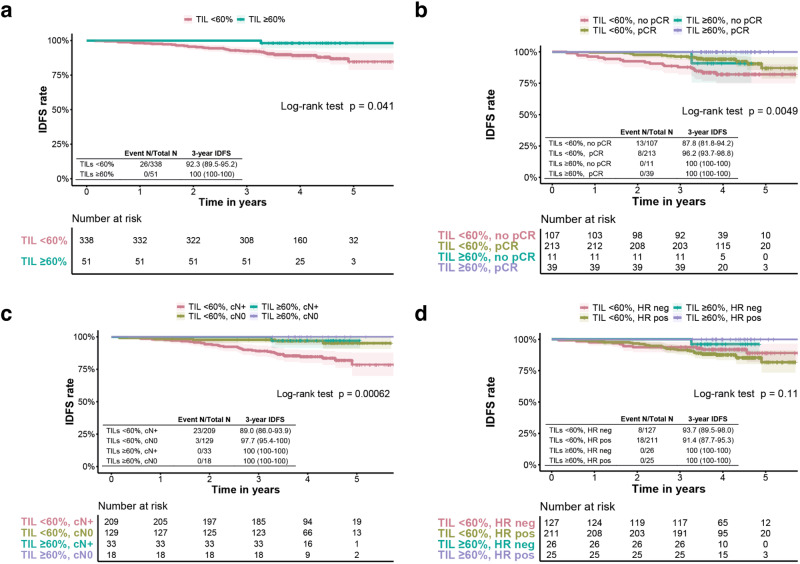
Tumor-infiltrating lymphocytes (TILs) have been associated with outcomes in HER2-positive breast cancer patients treated with neoadjuvant chemotherapy and trastuzumab. However, it remains unclear if TILs could be a prognostic and/or predictive biomarker in the context of dual HER2-targeting treatment. In this study, we evaluated the association between TILs and pathological response (pCR) and invasive-disease free survival (IDFS) in 389 patients with stage II-III HER2 positive breast cancer who received neoadjuvant anthracycline-containing or anthracycline-free chemotherapy combined with trastuzumab and pertuzumab in the TRAIN-2 trial. Although no significant association was seen between TILs and pCR, patients with TIL scores ≥60% demonstrated an excellent 3-year IDFS of 100% (95% CI 100-100), regardless of hormone receptor status, nodal stage and attainment of pCR. Additionally, in patients with hormone receptor positive disease, TILs as a continuous variable showed a trend to a positive association with pCR (adjusted Odds Ratio per 10% increase in TILs 1.15, 95% CI 0.99-1.34, p = 0.070) and IDFS (adjusted Hazard Ratio per 10% increase in TILs 0.71, 95% CI 0.50-1.01, p = 0.058). We found no interactions between TILs and anthracycline treatment. Our results suggest that high TIL scores might be able to identify stage II-III HER2-positive breast cancer patients with a favorable prognosis.
© 2024. The Author(s).
Conflict of interest statement
G.S.S. reports institutional research support from Agendia, AstraZeneca, Merck, Novartis, Roche and Seagen and consultancy fees paid to the institute from Biovica and Seagen. H.M.H. reports institutional research support from Roche. A.E.v.L. reports institutional research support from Agendia, AstraZeneca, Daiichi, Lilly, Novartis and Roche. L.M and R.B. were employees of Agendia NV at the time of analysis. The remaining authors declare no competing interests.
Figures
References
-
- van der Voort A, et al. Efficacy of neoadjuvant treatment with or without pertuzumab in patients with stage II and III HER2-positive breast cancer: a nationwide cohort analysis of pathologic response and 5-year survival. Breast. 2022;65:110–115. doi: 10.1016/j.breast.2022.07.005. - DOI - PMC - PubMed
-
- Schneeweiss A, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA) Ann. Oncol. 2013;24:2278–2284. doi: 10.1093/annonc/mdt182. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
