

Fourteen-day vonoprazan-based bismuth quadruple therapy for H. pylori eradication in an area with high clarithromycin and levofloxacin resistance: a prospective randomized study (VQ-HP trial)
- PMID: 38637591
- PMCID: PMC11026498
- DOI: 10.1038/s41598-024-59621-3
Fourteen-day vonoprazan-based bismuth quadruple therapy for H. pylori eradication in an area with high clarithromycin and levofloxacin resistance: a prospective randomized study (VQ-HP trial)
Abstract
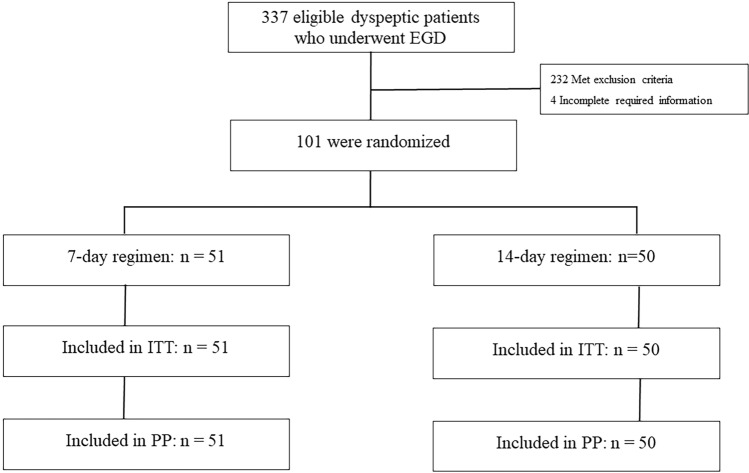
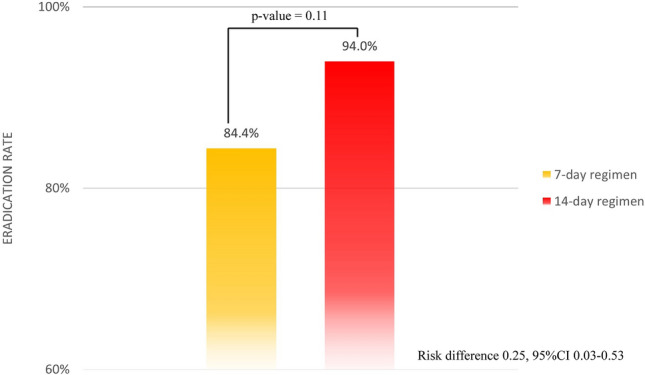
Potassium-competitive acid blockers (P-CABs) provide potent acid inhibition, yet studies on P-CAB-based quadruple therapy for H. pylori eradication are limited. We theorized that integrating bismuth subsalicylate into a quadruple therapy regimen could enhance eradication rates. However, data on the efficacy of vonoprazan bismuth quadruple therapy are notably scarce. Therefore, the aim of this study was to evaluate the efficacy of vonoprazan-based bismuth quadruple therapy in areas with high clarithromycin and levofloxacin resistance. This was a prospective, single-center, randomized trial conducted to compare the efficacy of 7-day and 14-day vonoprazan-based bismuth quadruple therapy for H. pylori eradication between June 1, 2021, and March 31, 2022. Qualified patients were randomly assigned to the 7-day or 14-day regimen (1:1 ratio by computer-generated randomized list as follows: 51 patients for the 7-day regimen and 50 patients for the 14-day regimen). The regimens consisted of vonoprazan (20 mg) twice daily, bismuth subsalicylate (1024 mg) twice daily, metronidazole (400 mg) three times daily, and tetracycline (500 mg) four times daily. CYP3A4/5 genotyping and antibiotic susceptibility tests were also performed. Successful eradication was defined as 13negative C-UBTs 4 weeks after treatment. The primary endpoint was to compare the efficacy of 7-day and 14-day regimens as first-line treatments, which were assessed by intention-to-treat (ITT) and per-protocol (PP) analyses. The secondary endpoints included adverse effects. A total of 337 dyspeptic patients who underwent gastroscopy were included; 105 patients (31.1%) were diagnosed with H. pylori infection, and 101 patients were randomly assigned to each regimen. No dropouts were detected. The antibiotic resistance rate was 33.3% for clarithromycin, 29.4% for metronidazole, and 27.7% for levofloxacin. The CYP3A4 genotype was associated with 100% rapid metabolism. The H. pylori eradication rates for the 7-day and 14-day regimens were 84.4%, 95% CI 74.3-94.2 and 94%, 95% CI 87.4-100, respectively (RR difference 0.25, 95% CI 0.03-0.53, p value = 0.11). Interestingly, the 14-day regimen led to 100% eradication in the clarithromycin-resistant group. Among the patients in the 7-day regimen group, only two exhibited resistance to clarithromycin; unfortunately, neither of them achieved a cure from H. pylori infection. The incidence of adverse events was similar in both treatment groups, occurring in 29.4% (15/51) and 28% (14/50) of patients in the 7-day and 14-day regimens, respectively. No serious adverse reactions were reported. In conclusion, 14 days of vonoprazan-based bismuth quadruple therapy is highly effective for H. pylori eradication in areas with high levels of dual clarithromycin and levofloxacin resistance.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
