

Development and validation of a new algorithm for improved cardiovascular risk prediction
- PMID: 38637635
- PMCID: PMC11108771
- DOI: 10.1038/s41591-024-02905-y
Development and validation of a new algorithm for improved cardiovascular risk prediction
Abstract
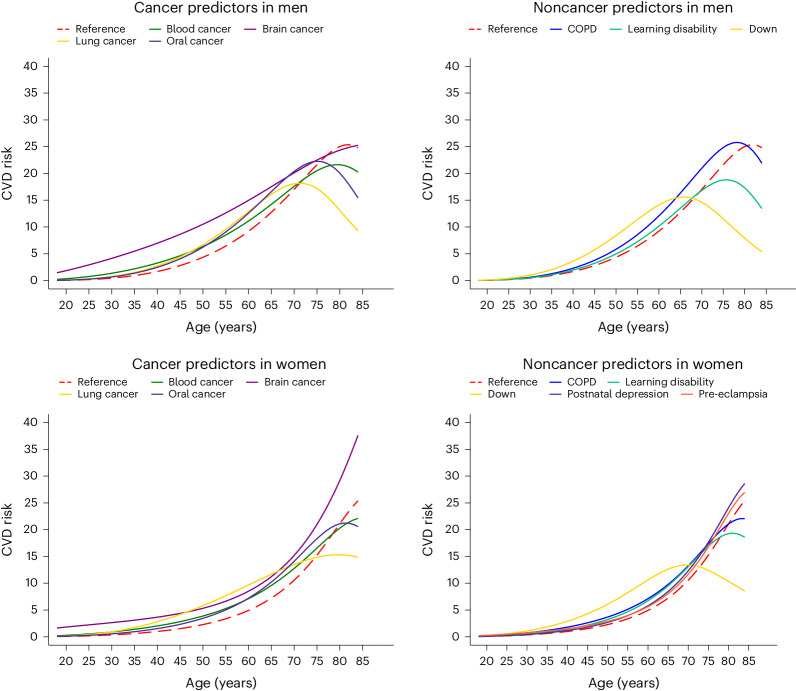
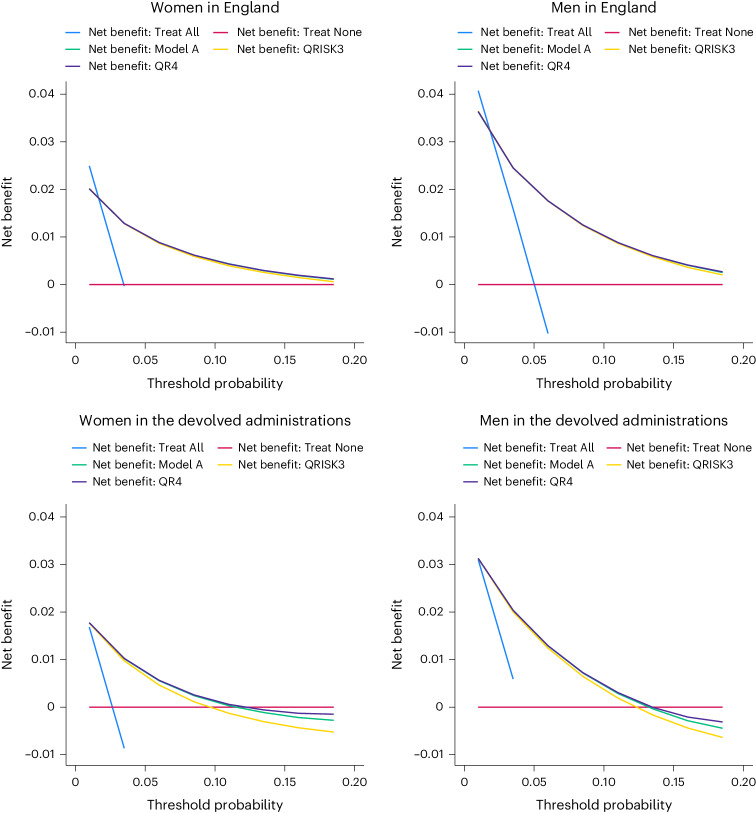
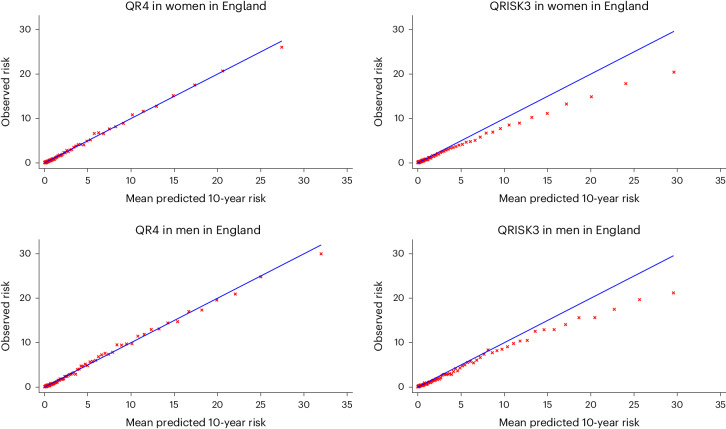
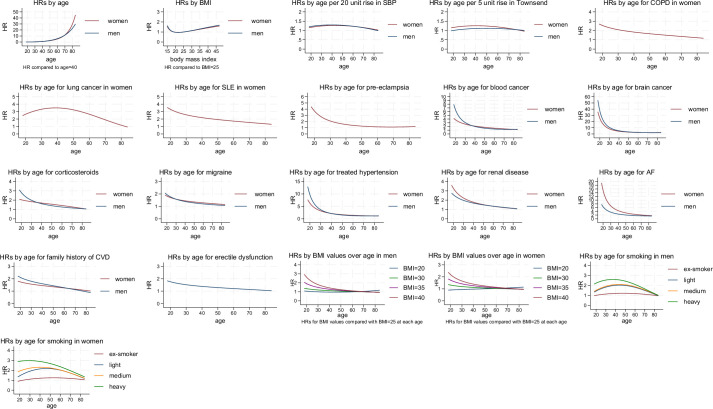
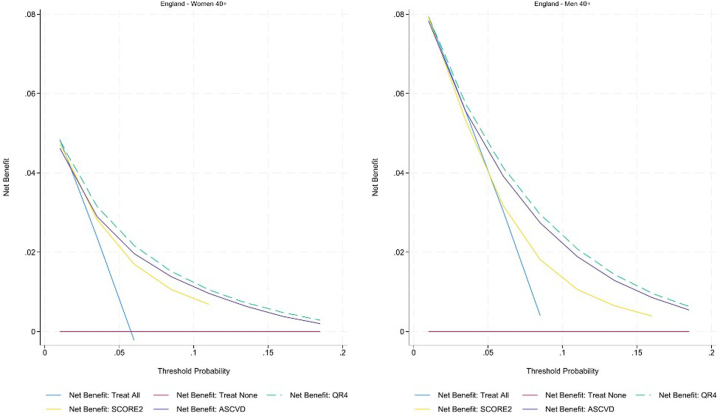
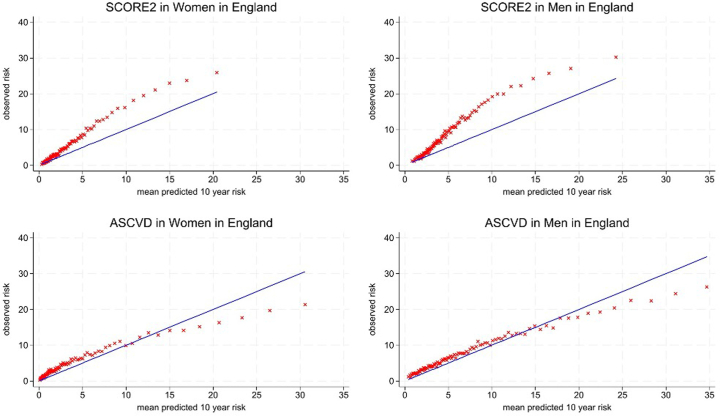
QRISK algorithms use data from millions of people to help clinicians identify individuals at high risk of cardiovascular disease (CVD). Here, we derive and externally validate a new algorithm, which we have named QR4, that incorporates novel risk factors to estimate 10-year CVD risk separately for men and women. Health data from 9.98 million and 6.79 million adults from the United Kingdom were used for derivation and validation of the algorithm, respectively. Cause-specific Cox models were used to develop models to predict CVD risk, and the performance of QR4 was compared with version 3 of QRISK, Systematic Coronary Risk Evaluation 2 (SCORE2) and atherosclerotic cardiovascular disease (ASCVD) risk scores. We identified seven novel risk factors in models for both men and women (brain cancer, lung cancer, Down syndrome, blood cancer, chronic obstructive pulmonary disease, oral cancer and learning disability) and two additional novel risk factors in women (pre-eclampsia and postnatal depression). On external validation, QR4 had a higher C statistic than QRISK3 in both women (0.835 (95% confidence interval (CI), 0.833-0.837) and 0.831 (95% CI, 0.829-0.832) for QR4 and QRISK3, respectively) and men (0.814 (95% CI, 0.812-0.816) and 0.812 (95% CI, 0.810-0.814) for QR4 and QRISK3, respectively). QR4 was also more accurate than the ASCVD and SCORE2 risk scores in both men and women. The QR4 risk score identifies new risk groups and provides superior CVD risk prediction in the United Kingdom compared with other international scoring systems for CVD risk.
© 2024. The Author(s).
Conflict of interest statement
All authors have completed the International Committee of Medical Journal Editors uniform disclosure form at
Figures

References
-
- Cardiovascular diseases (CVDs). World Health Organizationwww.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (2021).
-
- NICE Guideline [NG238]. Cardiovascular Disease: Risk Assessment and Reduction, Including Lipid Modification (National Institute for Clinical Excellence, 2023); www.nice.org.uk/guidance/ng238 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
