

Dynamics of clonal hematopoiesis under DNA-damaging treatment in patients with ovarian cancer
- PMID: 38637689
- PMCID: PMC11147769
- DOI: 10.1038/s41375-024-02253-3
Dynamics of clonal hematopoiesis under DNA-damaging treatment in patients with ovarian cancer
Erratum in
-
Correction: Dynamics of clonal hematopoiesis under DNA-damaging treatment in patients with ovarian cancer.Leukemia. 2024 Jun;38(6):1440. doi: 10.1038/s41375-024-02274-y. Leukemia. 2024. PMID: 38714878 Free PMC article. No abstract available.
Abstract
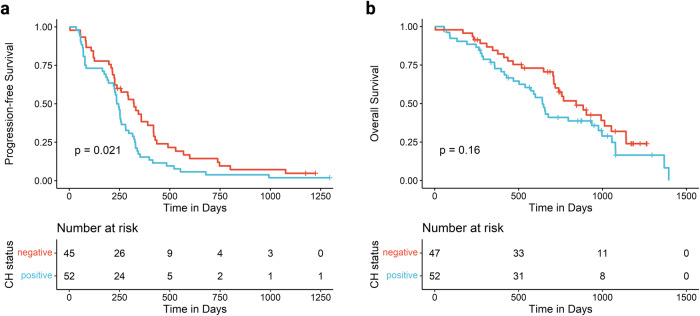
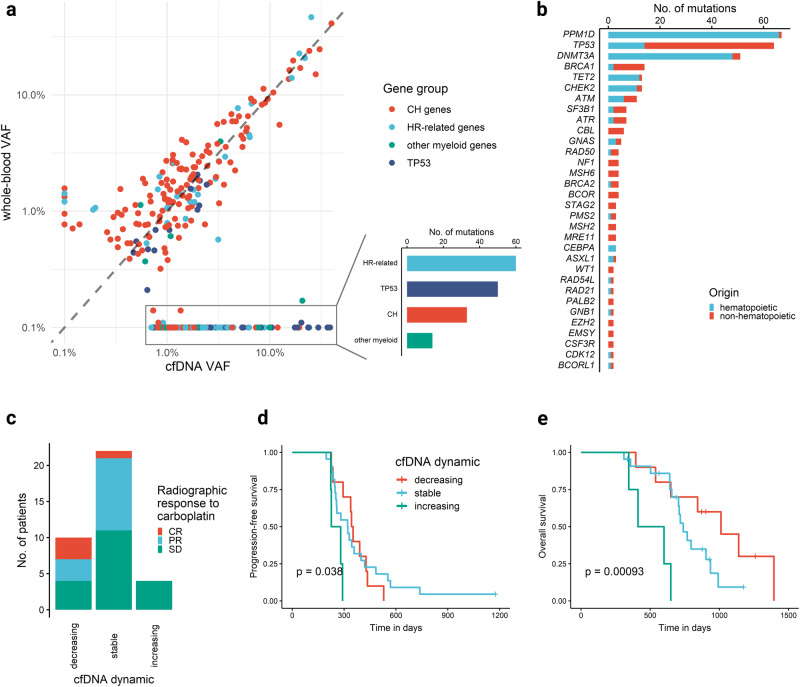
Clonal hematopoiesis (CH) driven by mutations in the DNA damage response (DDR) pathway is frequent in patients with cancer and is associated with a higher risk of therapy-related myeloid neoplasms (t-MNs). Here, we analyzed 423 serial whole blood and plasma samples from 103 patients with relapsed high-grade ovarian cancer receiving carboplatin, poly(ADP-ribose) polymerase inhibitor (PARPi) and heat shock protein 90 inhibitor (HSP90i) treatment within the phase II EUDARIO trial using error-corrected sequencing of 72 genes. DDR-driven CH was detected in 35% of patients and was associated with longer duration of prior PARPi treatment. TP53- and PPM1D-mutated clones exhibited substantially higher clonal expansion rates than DNMT3A- or TET2-mutated clones during treatment. Expansion of DDR clones correlated with HSP90i exposure across the three study arms and was partially abrogated by the presence of germline mutations related to homologous recombination deficiency. Single-cell DNA sequencing of selected samples revealed clonal exclusivity of DDR mutations, and identified DDR-mutated clones as the origin of t-MN in two investigated cases. Together, these results provide unique insights into the architecture and the preferential selection of DDR-mutated hematopoietic clones under intense DNA-damaging treatment. Specifically, PARPi and HSP90i therapies pose an independent risk for the expansion of DDR-CH in a dose-dependent manner.
© 2024. The Author(s).
Conflict of interest statement
FD reports personal fees from AbbVie, Amgen, Astra Zeneca, Gilead, Incyte, Novartis, and Roche outside the submitted work. LB reports advisory role for Abbvie, Amgen, Astellas, Bristol-Myers Squibb, Celgene, Daiichi Sankyo, Gilead, Hexal, Janssen, Jazz Pharmaceuticals, Menarini, Novartis, Pfizer, Sanofi, Servier; as well as research funding from Bayer, Jazz Pharmaceuticals. IR reports honoraria (personal) from Agenus, Blueprint, BMS, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche, GSK, MSD, Deciphera, Mersena, Merck Sereno, Novartis, Amgen, Macrogenics, Tesaro and Clovis; honoraria (institutional) from GSK, MSD, Roche and BMS; advisory/consulting fees from Abbvie, Agenus, Advaxis, BMS, ESAÏ, Daichi, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche/Genentech, GSK, MSD, Deciphera, Mersana, Merck Sereno, Novartis, Amgen, Tesaro and Clovis; research grant/funding (personal) from MSD, Roche and BMS; research grant/funding (institutional) from MSD, Roche, BMS, Novartis, Astra Zeneca and Merck Sereno; travel support from Roche, MSD, AstraZeneca and GSK. IV reports consulting fees from Agenus, AstraZeneca, Bristol Myers Squibb, Eisai, Genmab, GSK, Immunogen, Karyopharm, Mersana, MSD, Molecular Partners, Novocure, Novartis, Oncoinvent, Regeneron, Seagen, Verastem Oncology, Zai Lab, Zentalis. AGZ reports personal honoraria/travel supports from AbbVie, Amgen, Astra Zeneca, Eisai, Gilead, GSK, MSD, PharmaMar, Roche, Roche-Diagnostics Austria, Sandoz, outside the submitted work. WDS reports personal fees from AstraZeneca, GlaxoSmithKline, NOGGO and Roche outside the submitted work. All other authors declare no competing interests.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
