

Prevalence and differences in the co-administration of drugs known to interact: an analysis of three distinct and large populations
- PMID: 38637816
- PMCID: PMC11027217
- DOI: 10.1186/s12916-024-03384-1
Prevalence and differences in the co-administration of drugs known to interact: an analysis of three distinct and large populations
Abstract
Background: The co-administration of drugs known to interact greatly impacts morbidity, mortality, and health economics. This study aims to examine the drug-drug interaction (DDI) phenomenon with a large-scale longitudinal analysis of age and gender differences found in drug administration data from three distinct healthcare systems.
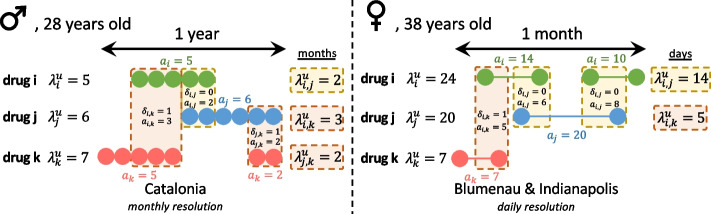
Methods: This study analyzes drug administrations from population-wide electronic health records in Blumenau (Brazil; 133 K individuals), Catalonia (Spain; 5.5 M individuals), and Indianapolis (USA; 264 K individuals). The stratified prevalences of DDI for multiple severity levels per patient gender and age at the time of administration are computed, and null models are used to estimate the expected impact of polypharmacy on DDI prevalence. Finally, to study actionable strategies to reduce DDI prevalence, alternative polypharmacy regimens using drugs with fewer known interactions are simulated.
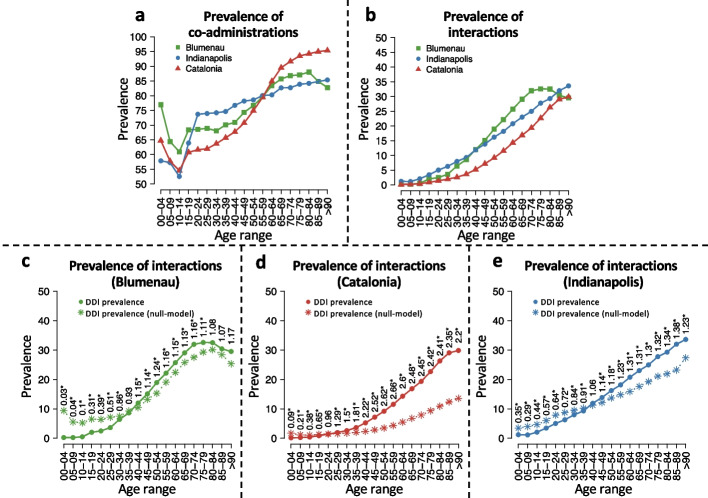
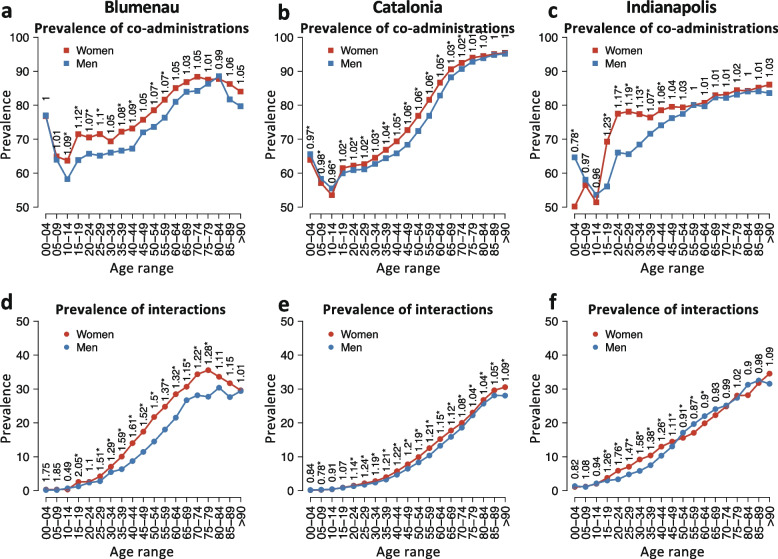
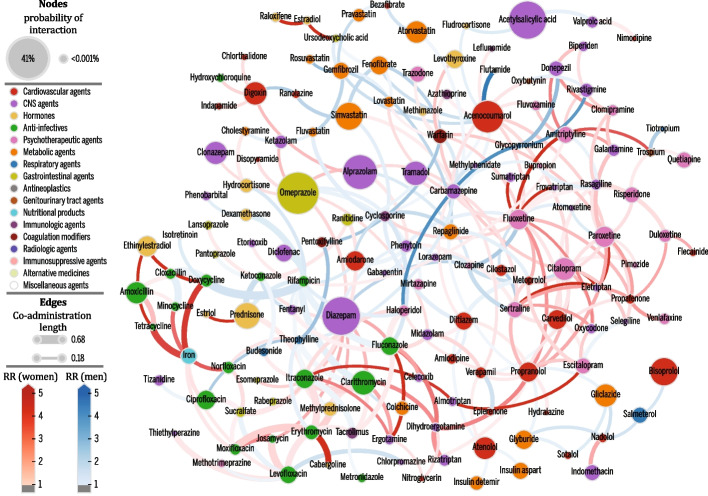
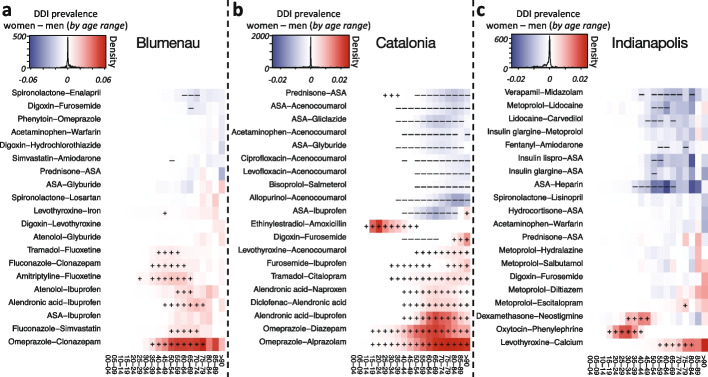
Results: A large prevalence of co-administration of drugs known to interact is found in all populations, affecting 12.51%, 12.12%, and 10.06% of individuals in Blumenau, Indianapolis, and Catalonia, respectively. Despite very different healthcare systems and drug availability, the increasing prevalence of DDI as patients age is very similar across all three populations and is not explained solely by higher co-administration rates in the elderly. In general, the prevalence of DDI is significantly higher in women - with the exception of men over 50 years old in Indianapolis. Finally, we show that using proton pump inhibitor alternatives to omeprazole (the drug involved in more co-administrations in Catalonia and Blumenau), the proportion of patients that are administered known DDI can be reduced by up to 21% in both Blumenau and Catalonia and 2% in Indianapolis.
Conclusions: DDI administration has a high incidence in society, regardless of geographic, population, and healthcare management differences. Although DDI prevalence increases with age, our analysis points to a complex phenomenon that is much more prevalent than expected, suggesting comorbidities as key drivers of the increase. Furthermore, the gender differences observed in most age groups across populations are concerning in regard to gender equity in healthcare. Finally, our study exemplifies how electronic health records' analysis can lead to actionable interventions that significantly reduce the administration of known DDI and its associated human and economic costs.
Keywords: Drug–drug interactions; Electronic health records; Multimorbidity; Polypharmacy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Update of
-
Analysis of electronic health records from three distinct and large populations reveals high prevalence and biases in the co-administration of drugs known to interact.medRxiv [Preprint]. 2023 Feb 8:2023.02.06.23285566. doi: 10.1101/2023.02.06.23285566. medRxiv. 2023. Update in: BMC Med. 2024 Apr 19;22(1):166. doi: 10.1186/s12916-024-03384-1. PMID: 36798425 Free PMC article. Updated. Preprint.
References
-
- Visser L. Hospitalisations and emergency department visits due to drug–drug interactions: a literature review. Pharmacoepidemiol Drug Saf. 2007;6(6):641–51. 10.1002/pds.1351. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
