

Autologous Pancreatic Islet Cell Transplantation Following Pancreatectomy for Pancreas Diseases Other Than Chronic Pancreatitis: A 15-y Study of the Milan Protocol
- PMID: 38637923
- PMCID: PMC11335085
- DOI: 10.1097/TP.0000000000005037
Autologous Pancreatic Islet Cell Transplantation Following Pancreatectomy for Pancreas Diseases Other Than Chronic Pancreatitis: A 15-y Study of the Milan Protocol
Abstract
Background: Pancreatogenic diabetes, a consequence of pancreatic tissue loss following pancreatectomy, poses a significant challenge for patients undergoing pancreatic surgery. Islet autotransplantation (IAT) offers a promising approach to prevent or alleviate pancreatogenic diabetes, but its application has been limited to individuals with painful chronic pancreatitis.
Methods: This study presents a 15-y clinical experience with the Milan Protocol, which expands IAT after pancreatectomy to a broader spectrum of patients with malignant and nonmalignant pancreatic diseases. The analysis evaluates feasibility, efficacy, and safety of IAT. Modified Igls criteria validated through the arginine test and mixed meal tolerance tests were used to assess long-term metabolic outcomes.
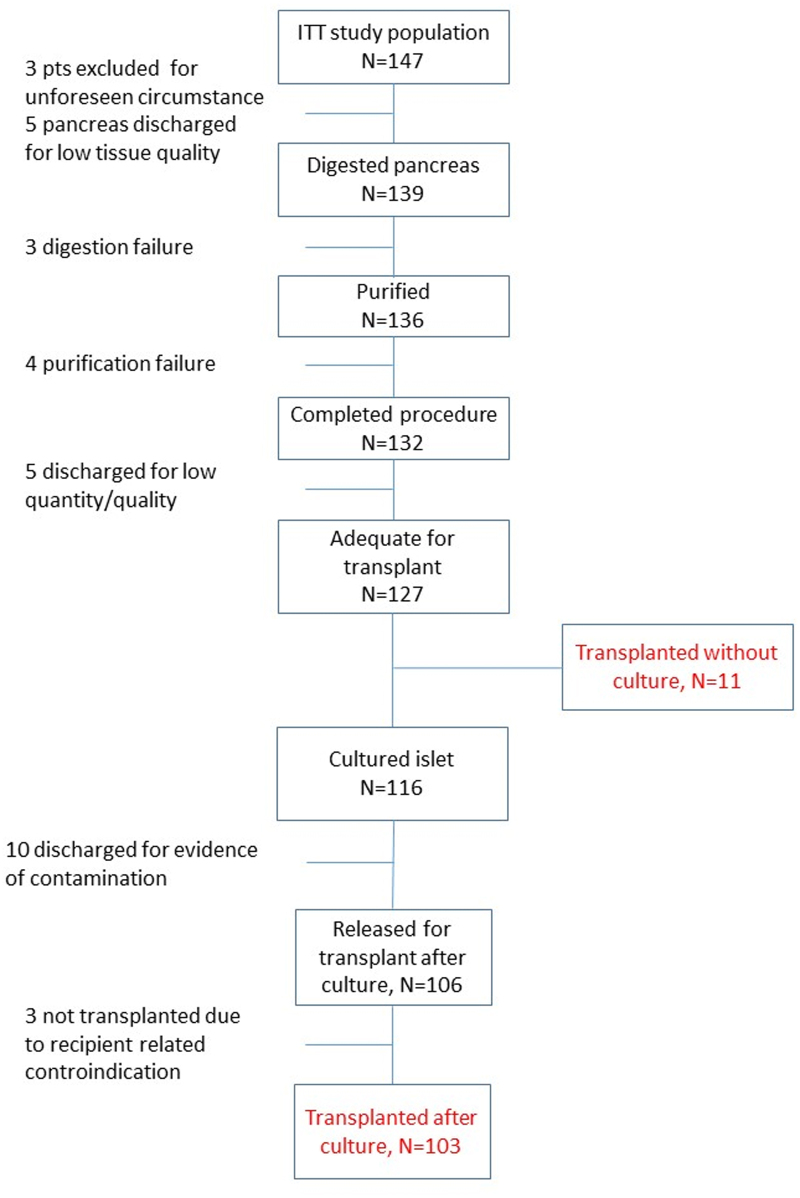
Results: Between November 2008 and June 2023, IAT procedures were performed on 114 of 147 candidates. IAT-related complications occurred in 19 of 114 patients (16.7%), with 5 being potentially serious. Patients exhibited sustained C-peptide secretion over the 10-y follow-up period, demonstrating a prevalence of optimal and good beta-cell function. Individuals who underwent partial pancreatectomy demonstrated superior metabolic outcomes, including sustained C-peptide secretion and a reduced risk of developing diabetes or insulin dependence compared with those who underwent total pancreatectomy. For patients who had total pancreatectomy, the quantity of infused islets and tissue volume were identified as critical factors influencing metabolic outcomes. An increased risk of recurrence or progression of baseline diseases was not observed in subjects with neoplasms.
Conclusions: These findings provide valuable insights into the benefits and applications of IAT as a therapeutic option for pancreatogenic diabetes after pancreatic surgery, expanding its potential beyond painful chronic pancreatitis.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






Comment in
-
Success With Islet Autotransplantation for Pancreatic Neoplasia Using a Careful Approach.Transplantation. 2024 Sep 1;108(9):1830-1831. doi: 10.1097/TP.0000000000005050. Epub 2024 May 21. Transplantation. 2024. PMID: 38771100 No abstract available.
References
-
- Infante M, Ricordi C. The unique pathophysiological features of diabetes mellitus secondary to total pancreatectomy: proposal for a new classification distinct from diabetes of the exocrine pancreas. Exp Rev Endocrinol Metab. 2023;18:19–32. - PubMed
-
- Reddy S, Wolfgang CL, Cameron JL, et al. . Total pancreatectomy for pancreatic adenocarcinoma: evaluation of morbidity and long-term survival. Ann Surg. 2009;250:282–287. - PubMed
-
- Hartwig W, Gluth A, Hinz U, et al. . Total pancreatectomy for primary pancreatic neoplasms: renaissance of an unpopular operation. Ann Surg. 2015;261:537–546. - PubMed
-
- Scavini M, Dugnani E, Pasquale V, et al. . Diabetes after pancreatic surgery: novel issues. Curr Diab Rep. 2015;15:16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
