

Enrichment of type 1 innate lymphoid cells in the course of human atherosclerotic plaque development suggests contribution to atherogenesis
- PMID: 38638438
- PMCID: PMC11024276
- DOI: 10.3389/fimmu.2024.1354617
Enrichment of type 1 innate lymphoid cells in the course of human atherosclerotic plaque development suggests contribution to atherogenesis
Abstract
Introduction: Innate lymphoid cells (ILCs) have been implicated in multiple pathologic conditions, including atherogenesis, as documented in experimental mice studies, however, their role in atherosclerosis in humans remains unexplored.
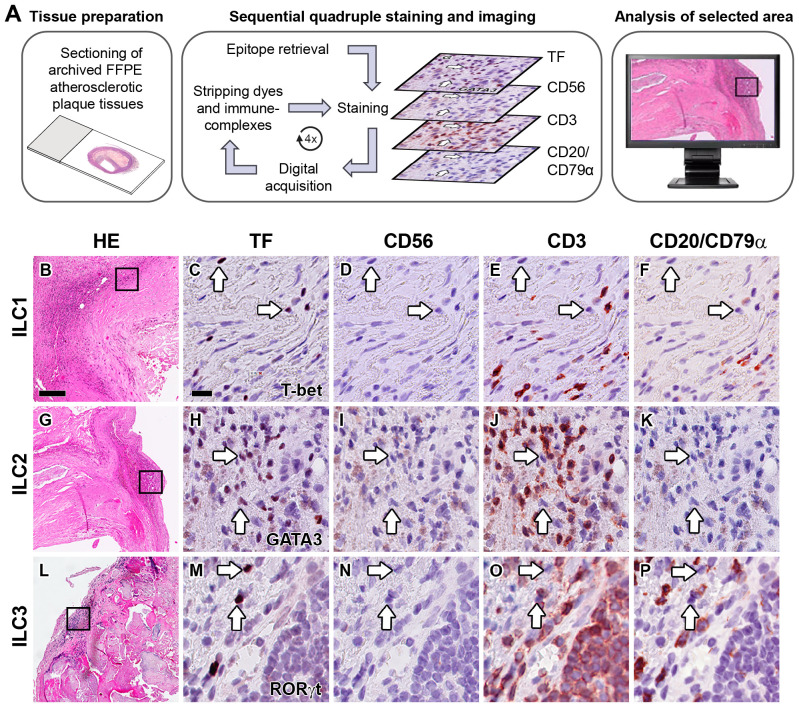
Methods: Here, we identify ILCs and their dynamics in early, advanced, and complicated human carotid- and aortic atherosclerotic plaques, using a multiplex immunohistochemical quadruple-staining technique with prototypic transcription factors T-bet, GATA3, or RORgt for identification of the ILC1, ILC2 and ILC3 subsets, respectively, in combination with lineage markers CD3, CD20/ CD79a and CD56 to exclude other lymphoid cell types. ILC subsets were quantified, and to put this in perspective, their numbers were expressed as percentage of the total number of infiltrated lymphoid cells and related to the frequency of conventional T cells, B cells, NK cells, and NKT cells.
Results: All ILC subsets were present in every different stage of atherogenesis. ILC1s were the most abundant ILC subset, and their numbers significantly increased in the course of plaque development, but paradoxically, their relative frequency was reduced because of a higher increment of T cells and B cells. The numbers of ILC2s and ILC3s also gradually increased, but this trend did not achieve significance. T cell subsets always significantly outnumbered their ILC counterparts, except for the early lesions where the proportion of ILC1s was markedly higher, albeit not significant.
Discussion: The high abundance of ILC1s in the early stages and further significant enrichment in later stages, suggest they may participate in the initiation and development of atherogenesis, and thus, may represent a novel target to prevent or treat atherosclerosis.
Keywords: atherosclerosis; immunohistochemistry; inflammation; innate immunity; innate lymphoid cells; lymphocytes.
Copyright © 2024 Pertiwi, Teunissen, Krebbers, Willems, Huisman, Poelen, van der Wal and de Boer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous