

Trends of Antihypertensive Prescription Among US Adults From 2010 to 2019 and Changes Following Treatment Guidelines: Analysis of Multicenter Electronic Health Records
- PMID: 38639340
- PMCID: PMC11179868
- DOI: 10.1161/JAHA.123.032197
Trends of Antihypertensive Prescription Among US Adults From 2010 to 2019 and Changes Following Treatment Guidelines: Analysis of Multicenter Electronic Health Records
Abstract
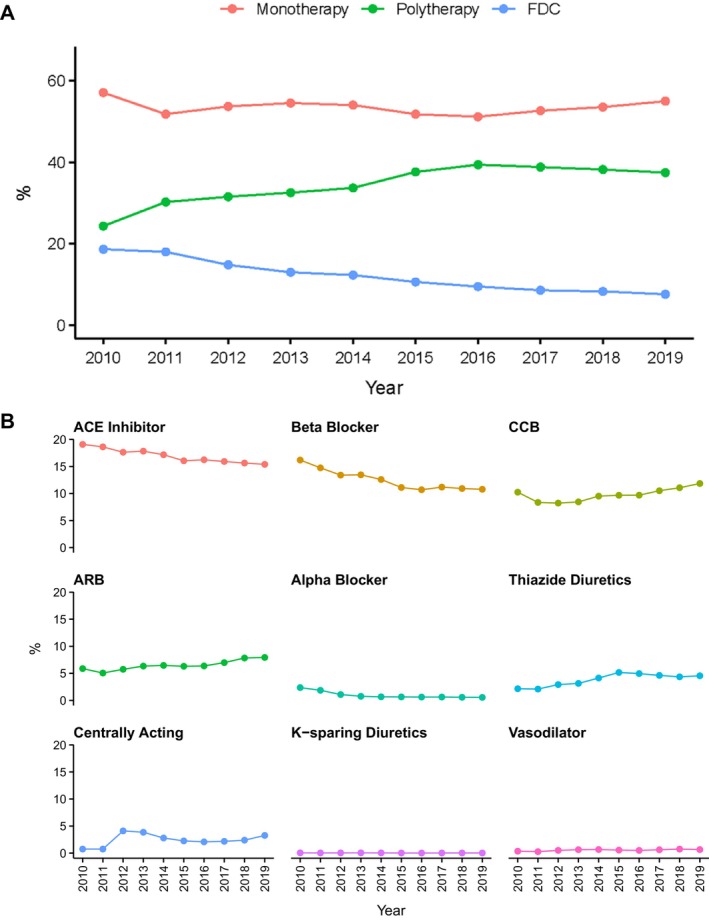
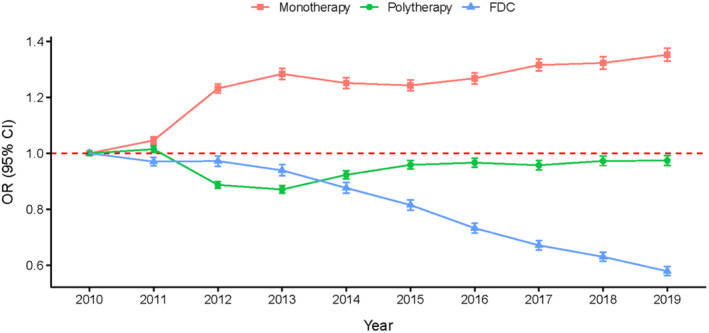
Background: Guidelines for the use of antihypertensives changed in 2014 and 2017. To understand the effect of these guidelines, we examined trends in antihypertensive prescriptions in the United States from 2010 to 2019 using a repeated cross-sectional design.
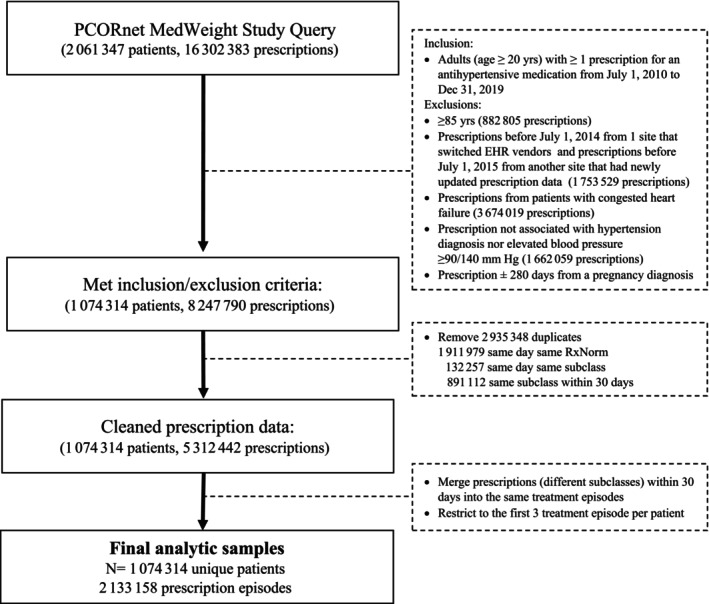
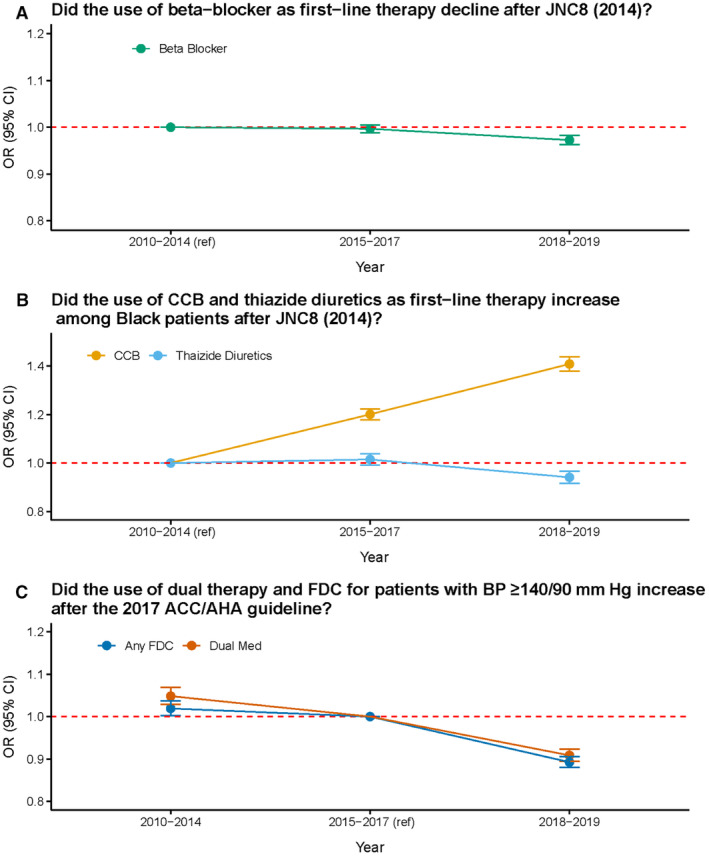
Methods and results: Using electronic health records from 15 health care institutions for adults (20-85 years old) who had ≥1 antihypertensive prescription, we assessed whether (1) prescriptions of beta blockers decreased after the 2014 Eighth Joint National Committee (JNC 8) report discouraged use for first-line treatment, (2) prescriptions for calcium channel blockers and thiazide diuretics increased among Black patients after the JNC 8 report encouraged use as first-line therapy, and (3) prescriptions for dual therapy and fixed-dose combination among patients with blood pressure ≥140/90 mm Hg increased after recommendations in the 2017 Hypertension Clinical Practice Guidelines. The study included 1 074 314 patients with 2 133 158 prescription episodes. After publication of the JNC 8 report, prescriptions for beta blockers decreased (3% lower in 2018-2019 compared to 2010-2014), and calcium channel blockers increased among Black patients (20% higher in 2015-2017 and 41% higher in 2018-2019, compared to 2010-2014), in accordance with guideline recommendations. However, contrary to guidelines, dual therapy and fixed-dose combination decreased after publication of the 2017 Hypertension Clinical Practice Guidelines (9% and 11% decrease in 2018-2019 for dual therapy and fixed-dose combination, respectively, compared to 2015-2017), and thiazide diuretics decreased among Black patients after the JNC 8 report (6% lower in 2018-2019 compared to 2010-2014).
Conclusions: Adherence to guidelines on prescribing antihypertensive medication was inconsistent, presenting an opportunity for interventions to achieve better blood pressure control in the US population.
Keywords: antihypertensive drugs; electronic health records; guideline adherence; prescriptions.
Figures
Similar articles
-
Potentially Inappropriate Antihypertensive Prescriptions to Elderly Patients: Results of a Prospective, Observational Study.Drugs Aging. 2017 Jun;34(6):453-466. doi: 10.1007/s40266-017-0452-z. Drugs Aging. 2017. PMID: 28432600
-
Evaluation of Prescription Pattern of Antihypertensives and Its Compliance with Joint National Committee 8 Guidelines in Hospital Setting.J Assoc Physicians India. 2024 Dec;72(12):e1-e5. doi: 10.59556/japi.72.0760. J Assoc Physicians India. 2024. PMID: 39676188
-
Guideline-directed antihypertensive medication use among young adult participants with uncontrolled hypertension at enrollment in the MyHEART study.BMC Cardiovasc Disord. 2024 Nov 13;24(1):636. doi: 10.1186/s12872-024-04313-z. BMC Cardiovasc Disord. 2024. PMID: 39538139 Free PMC article. Clinical Trial.
-
A critical appraisal of the guidelines from France, the UK, Europe and the USA for the management of hypertension in adults.Arch Cardiovasc Dis. 2015 Aug-Sep;108(8-9):453-9. doi: 10.1016/j.acvd.2015.05.006. Epub 2015 Jun 22. Arch Cardiovasc Dis. 2015. PMID: 26113481 Review.
-
[Practice of antihypertensive treatment in diabetic patients with hypertension in Hungary].Orv Hetil. 2014 Oct 26;155(43):1695-700. doi: 10.1556/OH.2014.29988. Orv Hetil. 2014. PMID: 25327459 Review. Hungarian.
Cited by
-
Blood Pressure-Elevating and Antihypertensive Medication Prescription Trends.Hypertension. 2025 Jun;82(6):1106-1115. doi: 10.1161/HYPERTENSIONAHA.124.24316. Epub 2025 Apr 22. Hypertension. 2025. PMID: 40326849 Free PMC article.
References
-
- Centers for Disease Control and Prevention . Hypertension cascade: hypertension prevalence, treatment and control estimates among U.S. Adults Aged 18 Years and Older Applying the Criteria from the American College of Cardiology and American Heart Association's 2017 Hypertension Guideline—NHANES 2017–2020. Centers for Disease Control and Prevention (CDC). Accessed May 12, 2023. https://millionhearts.hhs.gov/data‐reports/hypertension‐prevalence.html
-
- GBD 2015 Risk Factors Collaborators . Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1659–1724. doi: 10.1016/S0140-6736(16)31679-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
