

Newer Pharmacologic Treatments in Adults With Type 2 Diabetes: A Clinical Guideline From the American College of Physicians
- PMID: 38639546
- PMCID: PMC11614146
- DOI: 10.7326/M23-2788
Newer Pharmacologic Treatments in Adults With Type 2 Diabetes: A Clinical Guideline From the American College of Physicians
Abstract
Description: The American College of Physicians (ACP) developed this clinical guideline to update recommendations on newer pharmacologic treatments of type 2 diabetes. This clinical guideline is based on the best available evidence for effectiveness, comparative benefits and harms, consideration of patients' values and preferences, and costs.
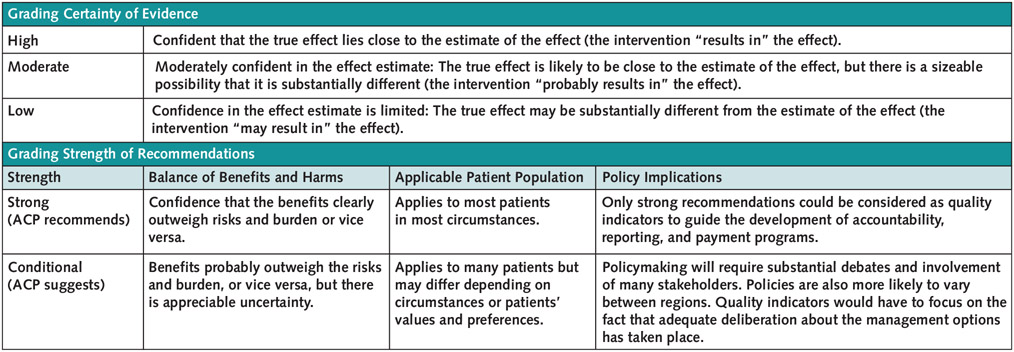
Methods: This clinical guideline is based on a systematic review of the effectiveness and harms of newer pharmacologic treatments of type 2 diabetes, including glucagon-like peptide-1 (GLP-1) agonists, a GLP-1 agonist and glucose-dependent insulinotropic polypeptide agonist, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, dipeptidyl peptidase-4 (DPP-4) inhibitors, and long-acting insulins, used either as monotherapy or in combination with other medications. The Clinical Guidelines Committee prioritized the following outcomes, which were evaluated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach: all-cause mortality, major adverse cardiovascular events, myocardial infarction, stroke, hospitalization for congestive heart failure, progression of chronic kidney disease, serious adverse events, and severe hypoglycemia. Weight loss, as measured by percentage of participants who achieved at least 10% total body weight loss, was a prioritized outcome, but data were insufficient for network meta-analysis and were not rated with GRADE.
Audience and patient population: The audience for this clinical guideline is physicians and other clinicians. The population is nonpregnant adults with type 2 diabetes.
Recommendation 1: ACP recommends adding a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or glucagon-like peptide-1 (GLP-1) agonist to metformin and lifestyle modifications in adults with type 2 diabetes and inadequate glycemic control (strong recommendation; high-certainty evidence). • Use an SGLT-2 inhibitor to reduce the risk for all-cause mortality, major adverse cardiovascular events, progression of chronic kidney disease, and hospitalization due to congestive heart failure. • Use a GLP-1 agonist to reduce the risk for all-cause mortality, major adverse cardiovascular events, and stroke.
Recommendation 2: ACP recommends against adding a dipeptidyl peptidase-4 (DPP-4) inhibitor to metformin and lifestyle modifications in adults with type 2 diabetes and inadequate glycemic control to reduce morbidity and all-cause mortality (strong recommendation; high-certainty evidence).
Conflict of interest statement
Figures



Comment in
-
Pharmacologic Treatments in Adults With Type 2 Diabetes: Cost-Effectiveness and Comorbidity Considerations.Ann Intern Med. 2024 May;177(5):680-681. doi: 10.7326/M24-0861. Epub 2024 Apr 19. Ann Intern Med. 2024. PMID: 38639544 No abstract available.
References
Web References
-
- American College of Physicians. Disclosure of interests and conflict of interest management summary for Clinical Guidelines Committee. 2023. Accessed at www.acponline.org/about-acp/who-we-are/leadership/boards-committees-coun... on 8 March 2024.
-
- Aluko P, Graybill E, Craig D, et al. Economic evidence. In: Higgins J, Thomas J, eds. Cochrane Handbook for Systematic Reviews of Interventions. 2022. Accessed at https://training.cochrane.org/handbook/current/chapter-20 on 8 March 2024.
-
- U.S. Centers for Medicare & Medicaid Services. Medicare Part D Spending by Drug. 2021. Accessed at https://data.cms.gov/summary-statistics-on-use-and-payments/medicare-med... on 8 March 2024.
References
-
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. 2023. Accessed at www.cdc.gov/diabetes/data/statistics-report/index.html on 8 March 2024.
-
- Cavender MA, Steg PG, Smith SC, et al.; REACH Registry Investigators. Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: outcomes at 4 years from the Reduction of Atherothrombosis for Continued Health (REACH) registry. Circulation. 2015;132:923–931. doi:10.1161/CIRCULATIONAHA.114.014796 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous