

Novel insights into the pathobiology of pulmonary hypertension in heart failure with preserved ejection fraction
- PMID: 38639739
- PMCID: PMC11380948
- DOI: 10.1152/ajpheart.00068.2024
Novel insights into the pathobiology of pulmonary hypertension in heart failure with preserved ejection fraction
Abstract
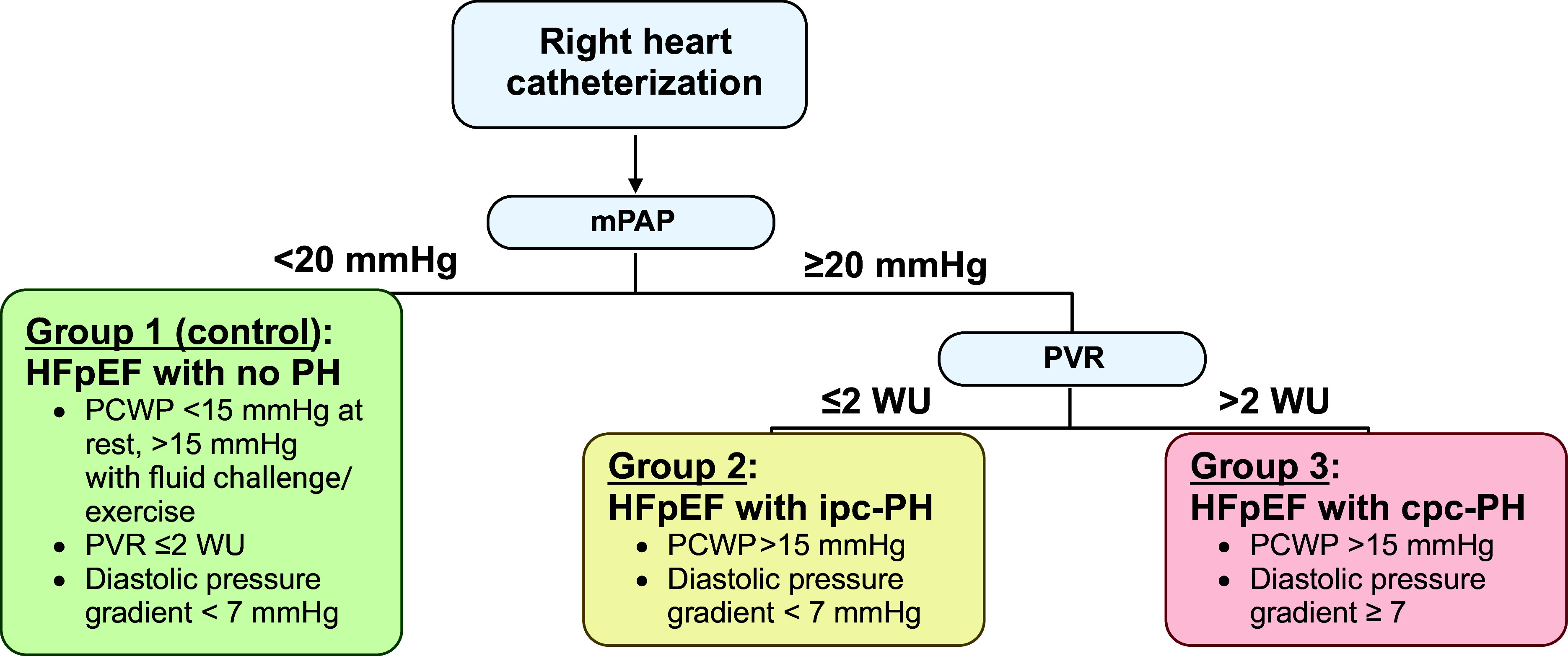
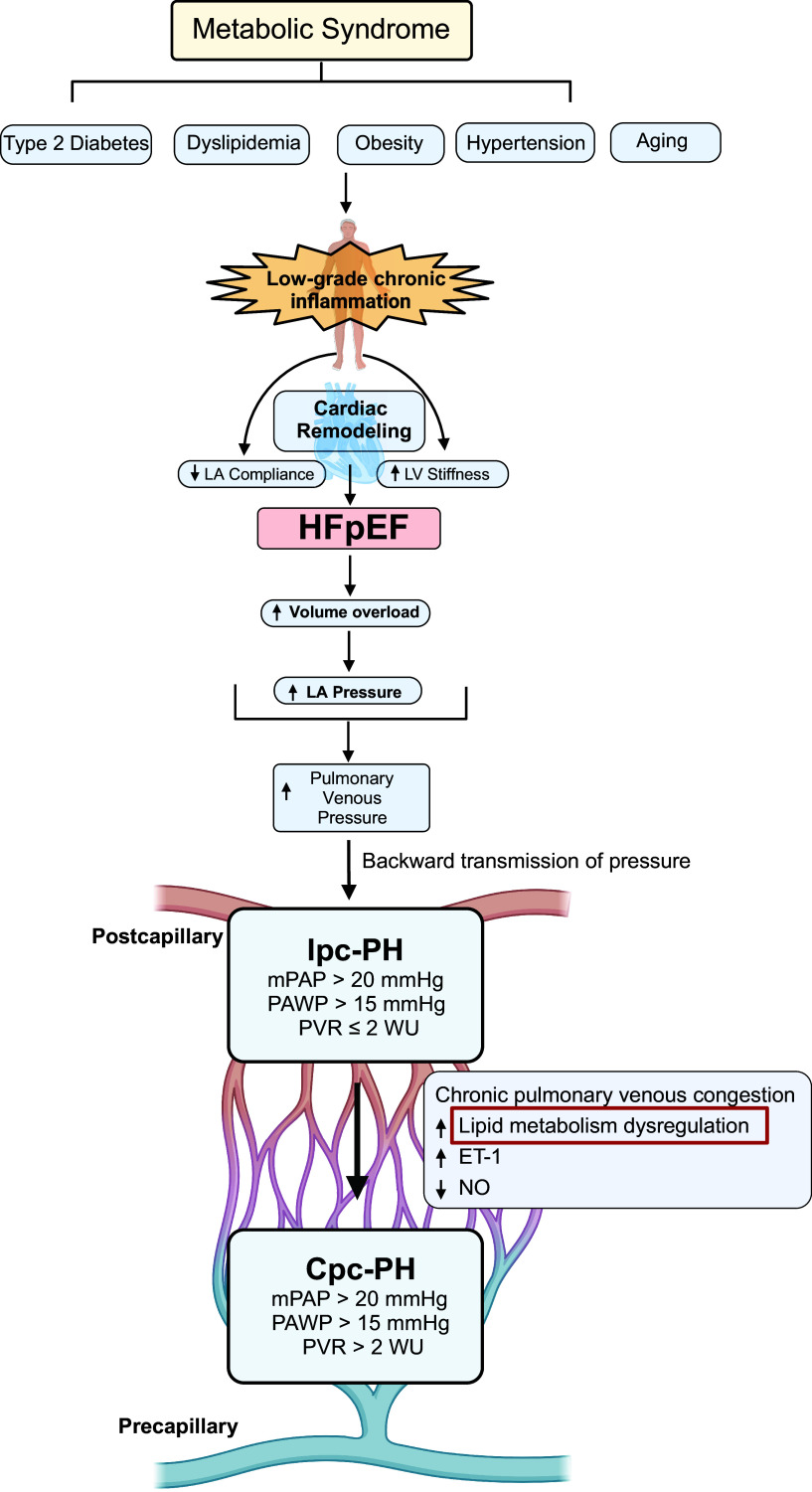
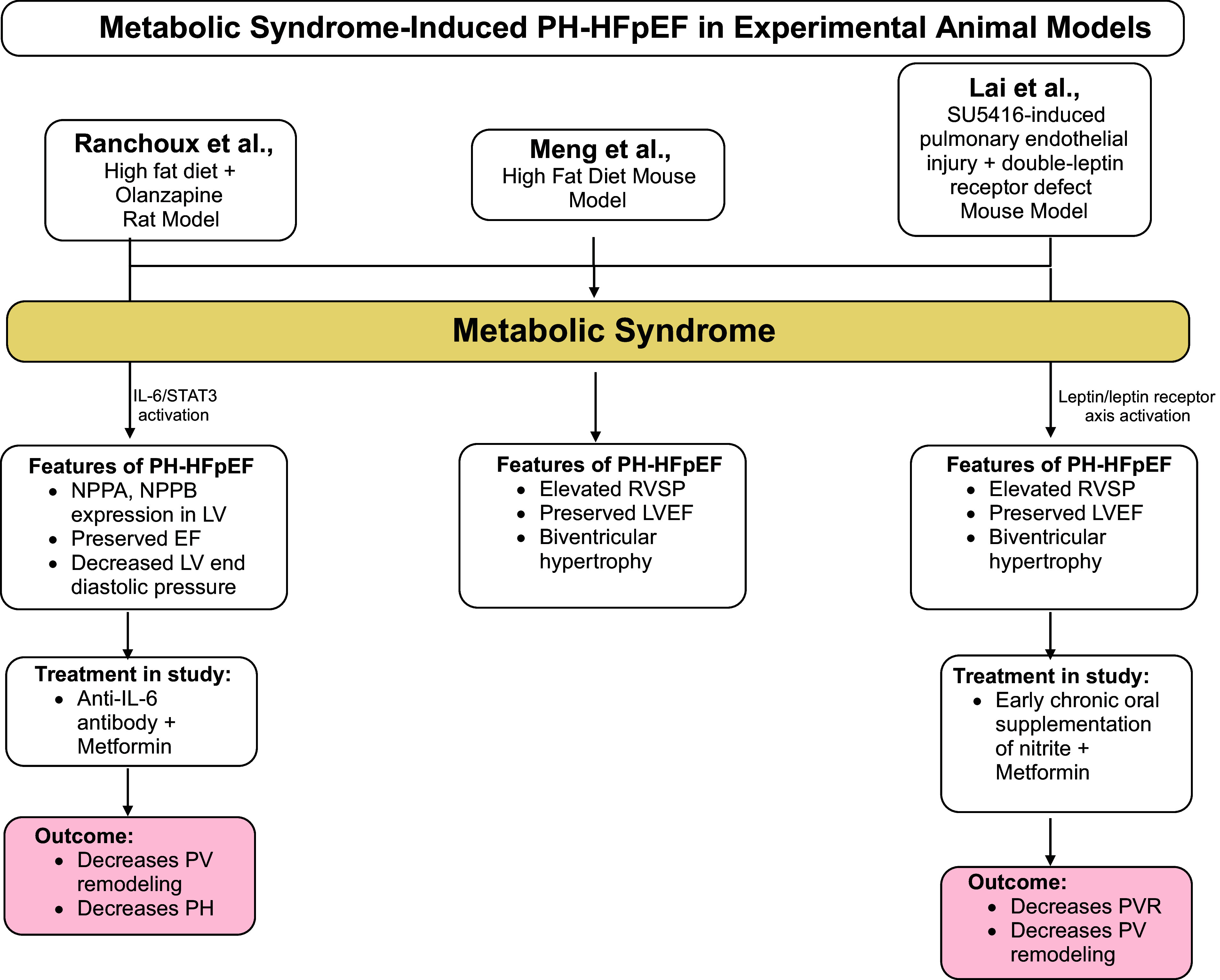
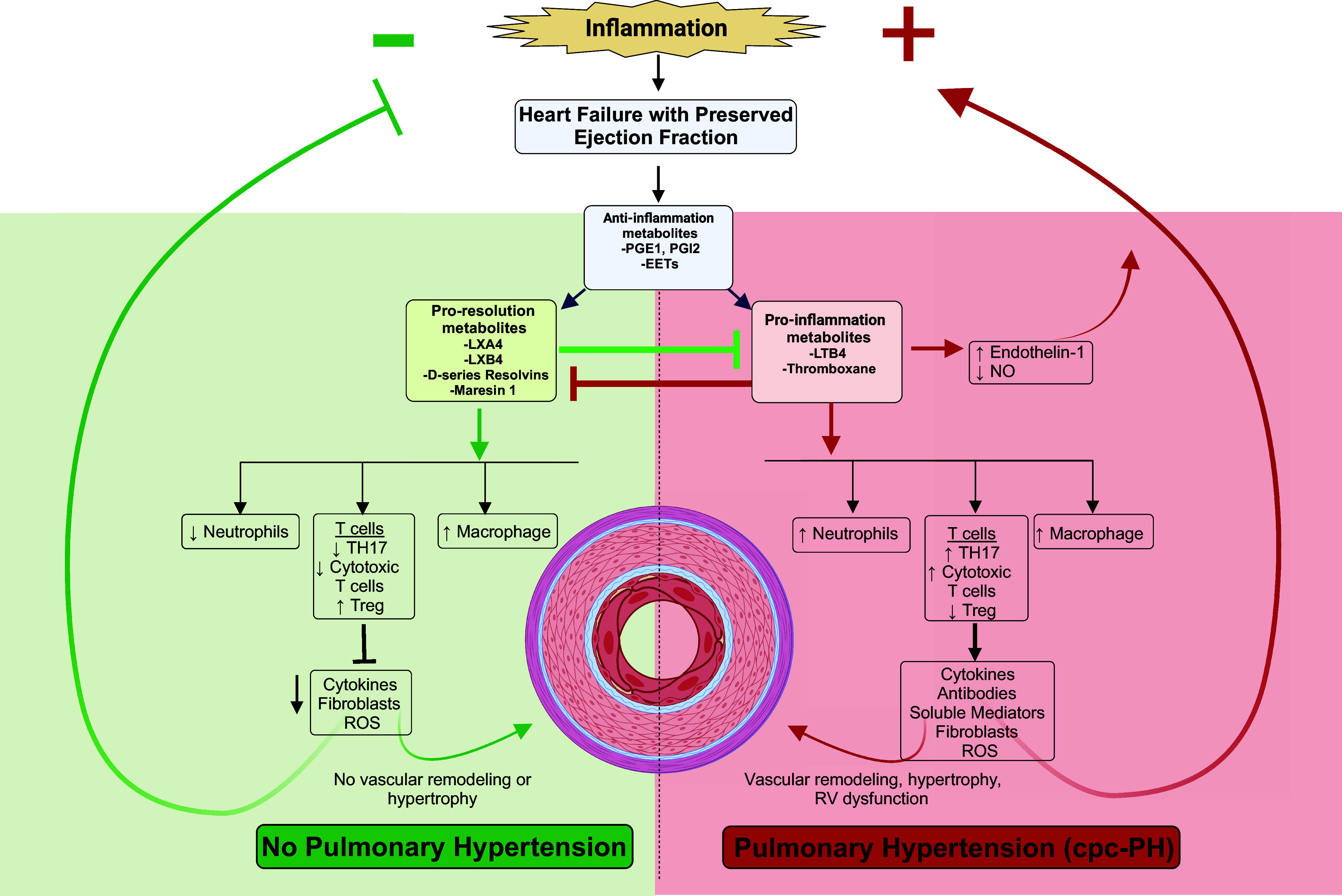
Heart failure (HF) with preserved ejection fraction (HFpEF) is the most common cause of pulmonary hypertension (PH) worldwide and is strongly associated with adverse clinical outcomes. The American Heart Association recently highlighted a call to action regarding the distinct lack of evidence-based treatments for PH due to poorly understood pathophysiology of PH attributable to HFpEF (PH-HFpEF). Prior studies have described cardiophysiological mechanisms to explain the development of isolated postcapillary PH (ipc-PH); however, the consequent increase in pulmonary vascular (PV) resistance (PVR) may lead to the less understood and more fatal combined pre- and postcapillary PH (cpc-PH). Metabolic disease and inflammatory dysregulation have been suggested to predispose PH, yet the molecular mechanisms are unknown. Although PH-HFpEF has been studied to partly share vasoactive neurohormonal mediators with primary pulmonary arterial hypertension (PAH), clinical trials that have targeted these pathways have been unsuccessful. The increased mortality of patients with PH-HFpEF necessitates further study into viable mechanistic targets involved in disease progression. We aim to summarize the current pathophysiological and clinical understanding of PH-HFpEF, highlight the role of known molecular mechanisms in the progression of PV disease, and introduce a novel concept that lipid metabolism may be attenuating and propagating PH-HFpEF.NEW & NOTEWORTHY Our review addresses pulmonary hypertension (PH) attributable to heart failure (HF) with preserved ejection fraction (HFpEF; PH-HFpEF). Current knowledge gaps in PH-HFpEF pathophysiology have led to a lack of therapeutic targets. Thus, we address identified knowledge gaps in a comprehensive review, focusing on current clinical epidemiology, known pathophysiology, and previously studied molecular mechanisms. We also introduce a comprehensive review of polyunsaturated fatty acid (PUFA) lipid inflammatory mediators in PH-HFpEF.
Keywords: HFpEF; PH; PH-HFpEF; PUFA; diastolic HF.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
Similar articles
-
Plasma Proteomics Identifies B2M as a Regulator of Pulmonary Hypertension in Heart Failure With Preserved Ejection Fraction.Arterioscler Thromb Vasc Biol. 2024 Jul;44(7):1570-1583. doi: 10.1161/ATVBAHA.123.320270. Epub 2024 May 30. Arterioscler Thromb Vasc Biol. 2024. PMID: 38813697 Free PMC article.
-
Pulmonary vascular disease in the setting of heart failure with preserved ejection fraction.Trends Cardiovasc Med. 2019 May;29(4):207-217. doi: 10.1016/j.tcm.2018.08.005. Epub 2018 Aug 17. Trends Cardiovasc Med. 2019. PMID: 30177249 Free PMC article. Review.
-
Skeletal Muscle SIRT3 Deficiency Contributes to Pulmonary Vascular Remodeling in Pulmonary Hypertension Due to Heart Failure With Preserved Ejection Fraction.Circulation. 2024 Sep 10;150(11):867-883. doi: 10.1161/CIRCULATIONAHA.124.068624. Epub 2024 May 28. Circulation. 2024. PMID: 38804138
-
Insights into the pulmonary vascular complications of heart failure with preserved ejection fraction.J Physiol. 2019 Feb;597(4):1143-1156. doi: 10.1113/JP275858. Epub 2018 Dec 30. J Physiol. 2019. PMID: 30549058 Free PMC article. Review.
-
Pulmonary hypertension secondary to heart failure with preserved ejection fraction.Can J Cardiol. 2015 Apr;31(4):430-9. doi: 10.1016/j.cjca.2014.12.028. Epub 2015 Jan 6. Can J Cardiol. 2015. PMID: 25840094 Review.
Cited by
-
Transcriptomic Analysis of Arachidonic Acid Pathway Genes Provides Mechanistic Insight into Multi-Organ Inflammatory and Vascular Diseases.Genes (Basel). 2024 Jul 20;15(7):954. doi: 10.3390/genes15070954. Genes (Basel). 2024. PMID: 39062733 Free PMC article.
-
Hemodynamic Definitions, Phenotypes, Pathophysiology, and Evaluation of Pulmonary Hypertension Related to Left Heart Disease.J Cardiovasc Dev Dis. 2025 Jun 22;12(7):238. doi: 10.3390/jcdd12070238. J Cardiovasc Dev Dis. 2025. PMID: 40710764 Free PMC article. Review.
References
-
- Shah SJ, Borlaug BA, Kitzman DW, McCulloch AD, Blaxall BC, Agarwal R, Chirinos JA, Collins S, Deo RC, Gladwin MT, Granzier H, Hummel SL, Kass DA, Redfield MM, Sam F, Wang TJ, Desvigne-Nickens P, Adhikari BB. Research priorities for heart failure with preserved ejection fraction: National Heart, Lung, and Blood Institute Working Group Summary. Circulation 141: 1001–1026, 2020. doi:10.1161/CIRCULATIONAHA.119.041886. - DOI - PMC - PubMed
-
- Brittain EL, Thenappan T, Huston JH, Agrawal V, Lai YC, Dixon D, Ryan JJ, Lewis EF, Redfield MM, Shah SJ, Maron BA; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Lifestyle and Cardiometabolic Health; and Stroke Council. Elucidating the clinical implications and pathophysiology of pulmonary hypertension in heart failure with preserved ejection fraction: a call to action: a science advisory from the American Heart Association. Circulation 146: e73–e88, 2022. doi:10.1161/CIR.0000000000001079. - DOI - PMC - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145: e876–e894, 2022. doi:10.1161/CIR.0000000000001062. - DOI - PubMed
-
- Prausmüller S, Weidenhammer A, Heitzinger G, Spinka G, Goliasch G, Arfsten H, Abdel Mawgoud R, Gabler C, Strunk G, Hengstenberg C, Hulsmann M, Bartko PE, Pavo N. Obesity in heart failure with preserved ejection fraction with and without diabetes: risk factor or innocent bystander? Eur J Prev Cardiol 30: 1247–1254, 2023. doi:10.1093/eurjpc/zwad140. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous