

ICG-Fluorescence Imaging for Margin Assessment During Minimally Invasive Colorectal Liver Metastasis Resection
- PMID: 38639939
- PMCID: PMC11031680
- DOI: 10.1001/jamanetworkopen.2024.6548
ICG-Fluorescence Imaging for Margin Assessment During Minimally Invasive Colorectal Liver Metastasis Resection
Abstract
Importance: Unintended tumor-positive resection margins occur frequently during minimally invasive surgery for colorectal liver metastases and potentially negatively influence oncologic outcomes.
Objective: To assess whether indocyanine green (ICG)-fluorescence-guided surgery is associated with achieving a higher radical resection rate in minimally invasive colorectal liver metastasis surgery and to assess the accuracy of ICG fluorescence for predicting the resection margin status.
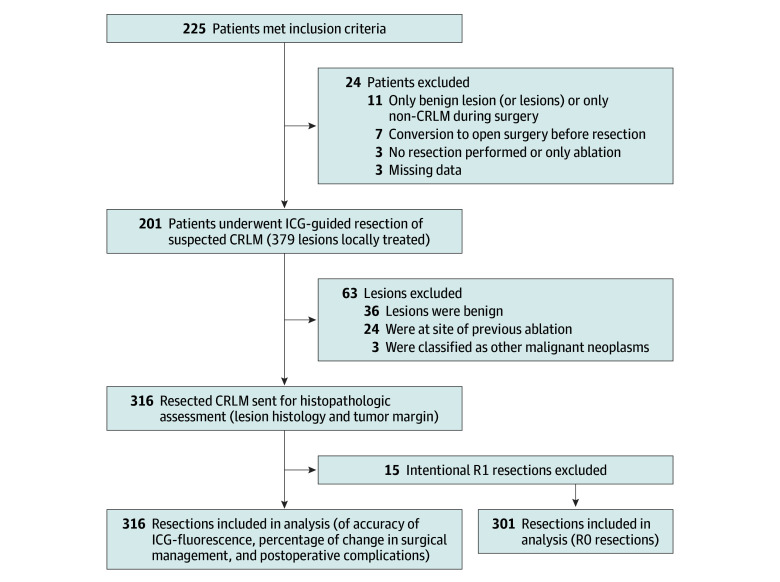
Design, setting, and participants: The MIMIC (Minimally Invasive, Indocyanine-Guided Metastasectomy in Patients With Colorectal Liver Metastases) trial was designed as a prospective single-arm multicenter cohort study in 8 Dutch liver surgery centers. Patients were scheduled to undergo minimally invasive (laparoscopic or robot-assisted) resections of colorectal liver metastases between September 1, 2018, and June 30, 2021.
Exposures: All patients received a single intravenous bolus of 10 mg of ICG 24 hours prior to surgery. During surgery, ICG-fluorescence imaging was used as an adjunct to ultrasonography and regular laparoscopy to guide and assess the resection margin in real time. The ICG-fluorescence imaging was performed during and after liver parenchymal transection to enable real-time assessment of the tumor margin. Absence of ICG fluorescence was favorable both during transection and in the tumor bed directly after resection.
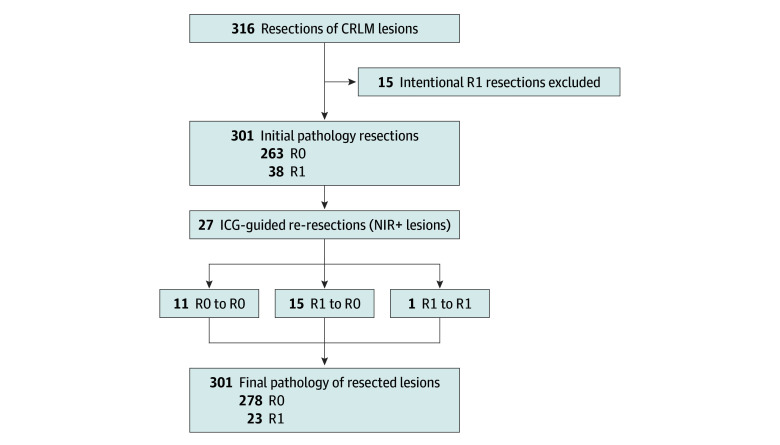
Main outcomes and measures: The primary outcome measure was the radical (R0) resection rate, defined by the percentage of colorectal liver metastases resected with at least a 1 mm distance between the tumor and resection plane. Secondary outcomes were the accuracy of ICG fluorescence in detecting margin-positive (R1; <1 mm margin) resections and the change in surgical management.
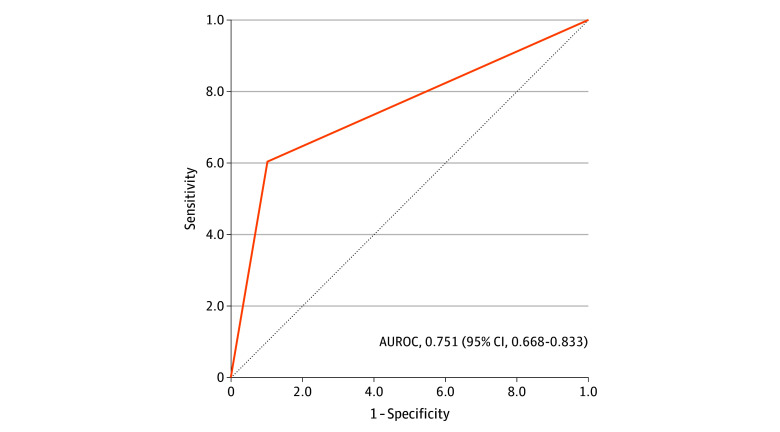
Results: In total, 225 patients were enrolled, of whom 201 (116 [57.7%] male; median age, 65 [IQR, 57-72] years) with 316 histologically proven colorectal liver metastases were included in the final analysis. The overall R0 resection rate was 92.4%. Re-resection of ICG-fluorescent tissue in the resection cavity was associated with a 5.0% increase in the R0 percentage (from 87.4% to 92.4%; P < .001). The sensitivity and specificity for real-time resection margin assessment were 60% and 90%, respectively (area under the receiver operating characteristic curve, 0.751; 95% CI, 0.668-0.833), with a positive predictive value of 54% and a negative predictive value of 92%. After training and proctoring of the first procedures, participating centers that were new to the technique had a comparable false-positive rate for predicting R1 resections during the first 10 procedures (odds ratio, 1.36; 95% CI, 0.44-4.24). The ICG-fluorescence imaging was associated with changes in intraoperative surgical management in 56 (27.9%) of the patients.
Conclusions and relevance: In this multicenter prospective cohort study, ICG-fluorescence imaging was associated with an increased rate of tumor margin-negative resection and changes in surgical management in more than one-quarter of the patients. The absence of ICG fluorescence during liver parenchymal transection predicted an R0 resection with 92% accuracy. These results suggest that use of ICG fluorescence may provide real-time feedback of the tumor margin and a higher rate of complete oncologic resection.
Conflict of interest statement
Figures
Comment in
References
-
- Cipriani F, Alzoubi M, Fuks D, et al. Pure laparoscopic versus open hemihepatectomy: a critical assessment and realistic expectations—a propensity score-based analysis of right and left hemihepatectomies from nine European tertiary referral centers. J Hepatobiliary Pancreat Sci. 2020;27(1):3-15. doi: 10.1002/jhbp.662 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
