

Gut-associated lymphoid tissue attrition associates with response to anti-α4β7 therapy in ulcerative colitis
- PMID: 38640252
- PMCID: PMC11140591
- DOI: 10.1126/sciimmunol.adg7549
Gut-associated lymphoid tissue attrition associates with response to anti-α4β7 therapy in ulcerative colitis
Abstract
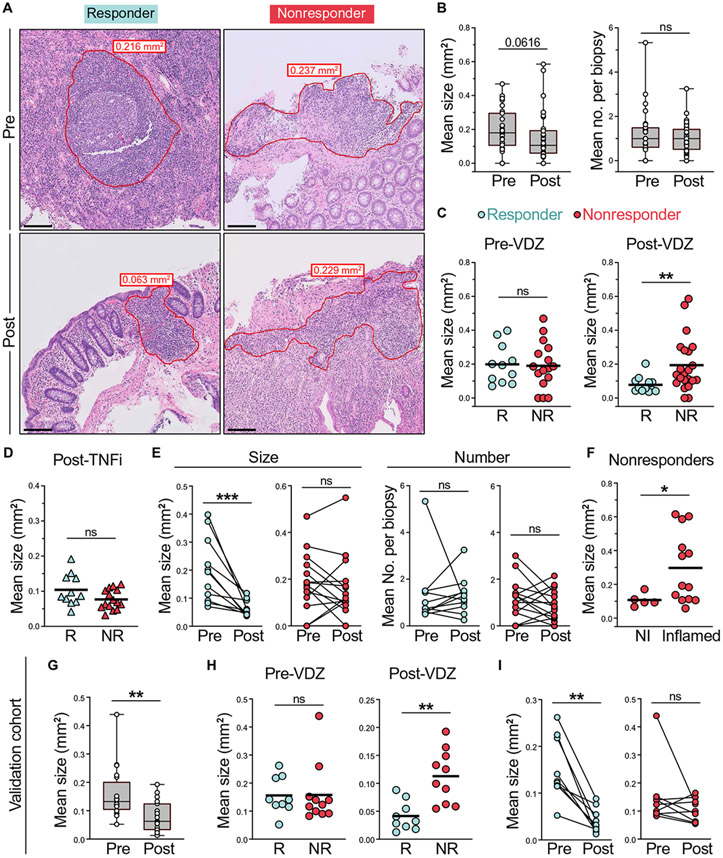
Vedolizumab (VDZ) is a first-line treatment in ulcerative colitis (UC) that targets the α4β7- mucosal vascular addressin cell adhesion molecule 1 (MAdCAM-1) axis. To determine the mechanisms of action of VDZ, we examined five distinct cohorts of patients with UC. A decrease in naïve B and T cells in the intestines and gut-homing (β7+) plasmablasts in circulation of VDZ-treated patients suggested that VDZ targets gut-associated lymphoid tissue (GALT). Anti-α4β7 blockade in wild-type and photoconvertible (KikGR) mice confirmed a loss of GALT size and cellularity because of impaired cellular entry. In VDZ-treated patients with UC, treatment responders demonstrated reduced intestinal lymphoid aggregate size and follicle organization and a reduction of β7+IgG+ plasmablasts in circulation, as well as IgG+ plasma cells and FcγR-dependent signaling in the intestine. GALT targeting represents a previously unappreciated mechanism of action of α4β7-targeted therapies, with major implications for this therapeutic paradigm in UC.
Figures






Update of
-
Gut-associated lymphoid tissue attrition associates with response to anti-α4β7 therapy in ulcerative colitis.bioRxiv [Preprint]. 2023 Jan 20:2023.01.19.524731. doi: 10.1101/2023.01.19.524731. bioRxiv. 2023. Update in: Sci Immunol. 2024 Apr 19;9(94):eadg7549. doi: 10.1126/sciimmunol.adg7549. PMID: 36711839 Free PMC article. Updated. Preprint.
References
-
- Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel J-F, Sandborn WJ, Van Assche G, Axler J, Kim H-J, Danese S, Fox I, Milch C, Sankoh S, Wyant T, Xu J, Parikh A, Vedolizumab as induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med 369, 699–710 (2013). - PubMed
-
- Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel J-F, Sands BE, Lukas M, Fedorak RN, Lee S, Bressler B, Fox I, Rosario M, Sankoh S, Xu J, Stephens K, Milch C, Parikh A, Vedolizumab as induction and maintenance therapy for Crohn’s disease. N. Engl. J. Med 369, 711–721 (2013). - PubMed
-
- Rott LS, Briskin MJ, Butcher EC, Expression of α4β7 and E-selectin ligand by circulating memory B cells: Implications for targeted trafficking to mucosal and systemic sites. J. Leukoc. Biol 68, 807–814 (2000). - PubMed
-
- Bargatze RF, Jutila MA, Butcher EC, Distinct roles of L-selectin and integrins alpha 4 beta 7 and LFA-1 in lymphocyte homing to Peyer's patch-HEV in situ: The multistep model confirmed and refined. Immunity 3, 99–108 (1995). - PubMed
-
- Lamb CA, O’Byrne S, Keir ME, Butcher EC, Gut-selective integrin-targeted therapies for inflammatory bowel disease. J. Crohns Colitis 12, S653–S668 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
