

Final phase 1 substudy results of ivosidenib for patients with mutant IDH1 relapsed/refractory myelodysplastic syndrome
- PMID: 38640348
- PMCID: PMC11372395
- DOI: 10.1182/bloodadvances.2023012302
Final phase 1 substudy results of ivosidenib for patients with mutant IDH1 relapsed/refractory myelodysplastic syndrome
Abstract
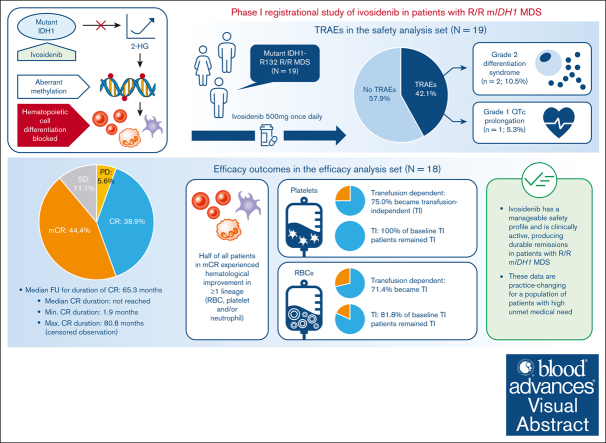
Ivosidenib is a first-in-class mutant isocitrate dehydrogenase 1 (mIDH1) inhibitor with efficacy and tolerability in patients with advanced mIDH1 hematologic malignancies, leading to approval in frontline and relapsed/refractory (R/R) mIDH1 acute myeloid leukemia. We report final data from a phase 1 single-arm substudy of once-daily ivosidenib in patients with R/R mIDH1 myelodysplastic syndrome (MDS) after failure of standard-of-care therapies. Primary objectives were to determine safety, tolerability, and clinical activity. The primary efficacy end point was the complete remission (CR) + partial remission (PR) rate. Nineteen patients were enrolled; 18 were included in the efficacy analysis. Treatment-related adverse events occurred in 8 (42.1%) patients, including a grade 1 QT interval prolongation in 1 (5.3%) patient and grade 2 differentiation syndrome in 2 (10.5%) patients. Rates of CR + PR and objective response (CR + PR + marrow CR) were 38.9% (95% confidence interval [CI], 17.3-64.3) and 83.3% (95% CI, 58.6-96.4), respectively. Kaplan-Meier estimates showed a 68.6% probability of patients in CR achieving a remission duration of ≥5 years, and a median overall survival of 35.7 months. Of note, 71.4% and 75.0% baseline red blood cell (RBC)- and platelet-transfusion-dependent patients, respectively, became transfusion independent (TI; no transfusion for ≥56 days); 81.8% and 100% of baseline RBC and platelet TI patients, respectively, remained TI. One (5.3%) patient proceeded to a hematopoietic stem cell transplant. In conclusion, ivosidenib is clinically active, with durable remissions and a manageable safety profile observed in these patients. This trial was registered at www.ClinicalTrials.gov as #NCT02074839.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: C.D.D. received research funding from AbbVie, Astex, ImmuneOnc, Bristol Myers Squibb, Cleave, Foghorn, Loxo, Rigel, Servier; consulting fees from Amgen, AbbVie, Astellas, Bristol Myers Squibb, GenMab, GlaxoSmithKline, Gilead, Jazz, Schrodinger, Servier, Stemline; honoraria for educational events from AbbVie, Astellas, Bristol Myers Squibb, Jazz, and Servier; meeting support from Servier; and has participated on a GenMab data safety board. G.J.R. has received consulting fees from Janssen, Amgen, Celgene, Novartis, Pfizer, AbbVie, Argenx, Jazz Pharmaceuticals, Roche, Daiichi Sankyo, Takeda, GlaxoSmithKline, Bristol Myers Squibb, Blueprint Medicines, bluebird bio, Jasper Pharmaceuticals, Syndax, Molecular Partners, Ellipses Pharma, AstraZeneca, Caribou and Rigel, and research funding from Janssen. J.M.W. has received consulting fees from Rigel, Servier; participated on safety monitoring or advisory boards for Rigel, Servier, Bristol Myers Squibb, Daiichi Sankyo, Aptose, Reven Pharma, and Rafael Pharma; and has received funding from Takeda and Immune Systems Key, Ltd. Y.F.M. has received consulting fees from GERON Pharmaceuticals, Kura Oncology, Blueprint Medicines, OncLive, MD Education, Sierra Oncology, Stemline Therapeutics, MorphoSys, Taiho Oncology, Rigel Pharmaceuticals, and Novartis, and support for attending meetings/travel from Blueprint Medicines, MD Education, and MorphoSys. P.B. has received consulting fees from MBS Pharma and ONO Pharmaceuticals; honoraria from Rigel Pharma and Bristol Myers Squibb; support for meetings/travel from KITE Pharma and Rigel Pharma; and has participated on data safety monitoring/advisory boards for Protagonist Therapeutics and KITE Pharma. S.d.B. has received support from Bristol Myers Squibb; research funding from Auron and Forma; consulting fees from Bristol Myers Squibb, GlaxoSmithKline, Remix, Servier, and Syndax; honoraria for speakers’ bureaus from AbbVie, Astellas, Bristol Myers Squibb, Jazz Pharmaceuticals, and Servier; honoraria from Loxo; and travel expenses from AbbVie and Servier. A.S. participated on speaker bureaus for Amgen and advisory boards for Sanofi and Daiichi-Sankyo. J.M.F. received institutional grants from Actinium, Astellas, Roivant, Celgene, Novartis, Takeda, Sellas, Kura, Pfizer, Servier, and Chordia; consulting fees from CTI Biopharma, Lava, Remix, Bristol Myers Squibb, and MJH LifeSciences; honoraria from Aptitude Health, AmerisourceBergen/IntrinsiQ Specialty Solutions, and MJH LifeSciences; is a member of the NCI Leukemia steering committee; and has stock options in Aurinia. D.A.S. has received consulting fees from AbbVie, Affimed, Gilead, Incyte, Intellisphere, Molecular Partners, PGEN Therapeutics, Takeda, and Zentalis; has participated on advisory boards for AvenCell, bluebird bio, Bristol Myers Squibb, Intellia, Jasper Therapeutics, KITE Pharma, Magenta Therapeutics, Nkarta, Novartis, Shattuck Labs, Servier, Syndax, and Syros; and reports payments from Aprea and Jazz were received by the Moffitt Cancer Center. D.M.M., M.H., X.B., P.A.P., and S.M.K. are employees of Servier, LLC. A.T.F. has received personal fees from Orum, Takeda, Servier, Amgen, Autolus, Rigel, Pfizer, Daiichi Sankyo, Forma, PureTech, EnClear, Genentech, Ipsen, AbbVie, Mablytics, Immunogen, Astellas, Bristol Myers Squibb/Celgene, Novartis, Agios, MorphoSys, Kite, Foghorn, Blueprint, Kura, and Trillium; and grants from AbbVie, Bristol Myers Squibb/Celgene, and Agios/Servier, outside the submitted work. The remaining authors declare no competing financial interests.
Figures





Comment in
-
This differentiation block will not stand, man: ivosidenib for MDS.Blood Adv. 2024 Aug 13;8(15):4207-4208. doi: 10.1182/bloodadvances.2024013427. Blood Adv. 2024. PMID: 39136969 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
