

A phase I study to evaluate the safety, pharmacokinetics, and pharmacodynamics of PF-06939999 (PRMT5 inhibitor) in patients with selected advanced or metastatic tumors with high incidence of splicing factor gene mutations
- PMID: 38640748
- PMCID: PMC11047177
- DOI: 10.1016/j.esmoop.2024.102961
A phase I study to evaluate the safety, pharmacokinetics, and pharmacodynamics of PF-06939999 (PRMT5 inhibitor) in patients with selected advanced or metastatic tumors with high incidence of splicing factor gene mutations
Abstract
Background: Protein arginine methyltransferase 5 (PRMT5) methylates multiple substrates dysregulated in cancer, including spliceosome machinery components. PF-06939999 is a selective small-molecule PRMT5 inhibitor.
Patients and methods: This phase I dose-escalation and -expansion trial (NCT03854227) enrolled patients with selected solid tumors. PF-06939999 was administered orally once or twice a day (q.d./b.i.d.) in 28-day cycles. The objectives were to evaluate PF-06939999 safety and tolerability to identify maximum tolerated dose (MTD) and recommended part 2 dose (RP2D), and assess pharmacokinetics (PK), pharmacodynamics [changes in plasma symmetric dimethylarginine (SDMA) levels], and antitumor activities.
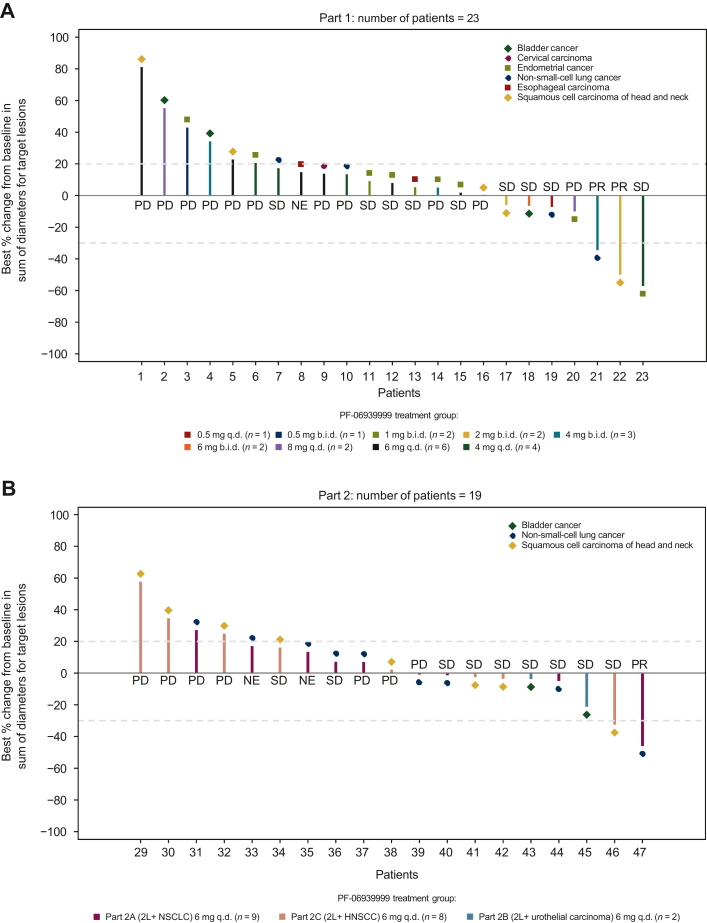
Results: In part 1 dose escalation, 28 patients received PF-06939999 (0.5 mg q.d. to 6 mg b.i.d.). Four of 24 (17%) patients reported dose-limiting toxicities: thrombocytopenia (n = 2, 6 mg b.i.d.), anemia (n = 1, 8 mg q.d.), and neutropenia (n = 1, 6 mg q.d.). PF-06939999 exposure increased with dose. Steady-state PK was achieved by day 15. Plasma SDMA was reduced at steady state (58%-88%). Modulation of plasma SDMA was dose dependent. No MTD was determined. In part 2 dose expansion, 26 patients received PF-06939999 6 mg q.d. (RP2D). Overall (part 1 + part 2), the most common grade ≥3 treatment-related adverse events included anemia (28%), thrombocytopenia/platelet count decreased (22%), fatigue (6%), and neutropenia (4%). Three patients (6.8%) had confirmed partial response (head and neck squamous cell carcinoma, n = 1; non-small-cell lung cancer, n = 2), and 19 (43.2%) had stable disease. No predictive biomarkers were identified.
Conclusions: PF-06939999 demonstrated a tolerable safety profile and objective clinical responses in a subset of patients, suggesting that PRMT5 is an interesting cancer target with clinical validation. However, no predictive biomarker was identified. The role of PRMT5 in cancer biology is complex and requires further preclinical, mechanistic investigation to identify predictive biomarkers for patient selection.
Keywords: PF-06939999; PRMT5 inhibitor; dose escalation; dose expansion; phase I; solid tumors.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Jensen-Pergakes K., Tatlock J., Maegley K.A., et al. SAM-competitive PRMT5 inhibitor PF-06939999 demonstrates antitumor activity in splicing dysregulated NSCLC with decreased liability of drug resistance. Mol Cancer Ther. 2022;21(1):3–15. - PubMed
-
- Rodon J., Perez C.A., Wong K.M., et al. PF-06939999, a potent and selective PRMT5 inhibitor, in patients with advanced or meta-static solid tumors: a phase 1 dose escalation study. J Clin Oncol. 2021;39:3019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
