

Ninety-Day Stroke Recurrence in Minor Stroke: Systematic Review and Meta-Analysis of Trials and Observational Studies
- PMID: 38641856
- PMCID: PMC11179866
- DOI: 10.1161/JAHA.123.032471
Ninety-Day Stroke Recurrence in Minor Stroke: Systematic Review and Meta-Analysis of Trials and Observational Studies
Abstract
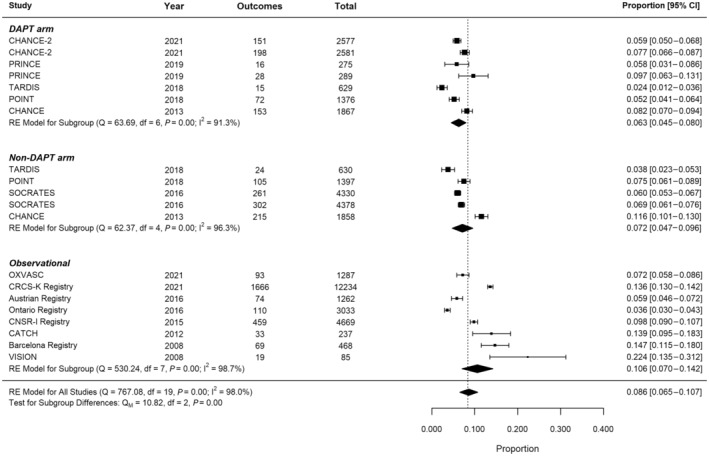
Background: Risk of recurrence after minor ischemic stroke is usually reported with transient ischemic attack. No previous meta-analysis has focused on minor ischemic stroke alone. The objective was to evaluate the pooled proportion of 90-day stroke recurrence for minor ischemic stroke, defined as a National Institutes of Health Stroke Scale severity score of ≤5.
Methods and results: Published papers found on PubMed from 2000 to January 12, 2021, reference lists of relevant articles, and experts in the field were involved in identifying relevant studies. Randomized controlled trials and observational studies describing minor stroke cohort with reported 90-day stroke recurrence were selected by 2 independent reviewers. Altogether 14 of 432 (3.2%) studies met inclusion criteria. Multilevel random-effects meta-analysis was performed. A total of 6 randomized controlled trials and 8 observational studies totaling 45 462 patients were included. The pooled 90-day stroke recurrence was 8.6% (95% CI, 6.5-10.7), reducing by 0.60% (95% CI, 0.09-1.1; P=0.02) with each subsequent year of publication. Recurrence was lowest in dual antiplatelet trial arms (6.3%, 95% CI, 4.5-8.0) when compared with non-dual antiplatelet trial arms (7.2%, 95% CI, 4.7-9.6) and observational studies 10.6% (95% CI, 7.0-14.2). Age, hypertension, diabetes, ischemic heart disease, or known atrial fibrillation had no significant association with outcome. Defining minor stroke with a lower National Institutes of Health Stroke Scale threshold made no difference - score ≤3: 8.6% (95% CI, 6.0-11.1), score ≤4: 8.4% (95% CI, 6.1-10.6), as did excluding studies with n<500%-7.3% (95% CI, 5.5-9.0).
Conclusions: The risk of recurrence after minor ischemic stroke is declining over time but remains important.
Keywords: humans; ischemic attack, transient; recurrence; stroke.
Figures
Similar articles
-
Dual versus mono antiplatelet therapy for acute non-cardioembolic ischaemic stroke or transient ischaemic attack: a systematic review and meta-analysis.Stroke Vasc Neurol. 2018 Jun 26;3(2):107-116. doi: 10.1136/svn-2018-000168. eCollection 2018 Jun. Stroke Vasc Neurol. 2018. PMID: 30022798 Free PMC article.
-
Clopidogrel with indobufen or aspirin in minor ischemic stroke or high-risk transient ischemic attack: a randomized controlled clinical study.BMC Neurol. 2024 Mar 1;24(1):81. doi: 10.1186/s12883-024-03585-4. BMC Neurol. 2024. PMID: 38429754 Free PMC article. Clinical Trial.
-
Meta-analysis of patent foramen ovale closure versus medical therapy for prevention of recurrent ischemic neurological events: Impact of medication type.Medicine (Baltimore). 2021 Jun 25;100(25):e26473. doi: 10.1097/MD.0000000000026473. Medicine (Baltimore). 2021. PMID: 34160457 Free PMC article.
-
Disability After Minor Stroke and Transient Ischemic Attack in the POINT Trial.Stroke. 2020 Mar;51(3):792-799. doi: 10.1161/STROKEAHA.119.027465. Epub 2020 Feb 12. Stroke. 2020. PMID: 32078486 Free PMC article.
-
[Meta-analysis on the efficacy and adverse events of aspirin plus clopidogrel versus aspirin-monotherapy in patients with ischemic stroke or transient ischemic attack].Zhonghua Liu Xing Bing Xue Za Zhi. 2015 Dec;36(12):1430-5. Zhonghua Liu Xing Bing Xue Za Zhi. 2015. PMID: 26850406 Chinese.
Cited by
-
Analysis of Non-Cardiogenic Young Minor Ischemic Stroke Patients' Risk Factors in Chinese Han Population.Med Sci Monit. 2025 Feb 1;31:e946146. doi: 10.12659/MSM.946146. Med Sci Monit. 2025. PMID: 39891380 Free PMC article.
-
Non-high-density Lipoprotein Cholesterol for Secondary Prevention after Minor Stroke.J Atheroscler Thromb. 2025 Feb 1;32(2):122-124. doi: 10.5551/jat.ED272. Epub 2024 Nov 16. J Atheroscler Thromb. 2025. PMID: 39551491 Free PMC article. No abstract available.
-
Impact of dual antiplatelet therapy on patients with minor stroke after thrombolysis: a systematic review and meta-analysis.BMJ Neurol Open. 2025 Mar 12;7(1):e000957. doi: 10.1136/bmjno-2024-000957. eCollection 2025. BMJ Neurol Open. 2025. PMID: 40099164 Free PMC article.
-
Intravenous thrombolysis or antiplatelet therapy for acute nondisabling ischemic stroke: A systematic review and network meta-analysis.Eur Stroke J. 2025 Jun;10(2):330-338. doi: 10.1177/23969873241293323. Epub 2024 Oct 26. Eur Stroke J. 2025. PMID: 39460567 Free PMC article.
-
The impact of periodic leg movements during sleep on neurological recovery in patients with acute mild cerebral infarction.Front Neurol. 2025 Aug 1;16:1610871. doi: 10.3389/fneur.2025.1610871. eCollection 2025. Front Neurol. 2025. PMID: 40823310 Free PMC article.
References
-
- Wang Y, Chen W, Lin Y, Meng X, Chen G, Wang Z, Wu J, Wang D, Li J, Cao Y. Ticagrelor plus aspirin versus clopidogrel plus aspirin for platelet reactivity in patients with minor stroke or transient ischaemic attack: open label, blinded endpoint, randomised controlled phase II trial. BMJ. 2019;365:l2211. - PMC - PubMed
-
- Bath PM, Woodhouse LJ, Appleton JP, Beridze M, Christensen H, Dineen RA, Flaherty K, Duley L, England TJ, Havard D, et al. Triple versus guideline antiplatelet therapy to prevent recurrence after acute ischaemic stroke or transient ischaemic attack: the TARDIS RCT. Health Technol Assess. 2018;22:1–76. doi: 10.3310/hta22480 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
