

The Immunology of Psoriasis-Current Concepts in Pathogenesis
- PMID: 38642273
- PMCID: PMC11193704
- DOI: 10.1007/s12016-024-08991-7
The Immunology of Psoriasis-Current Concepts in Pathogenesis
Abstract
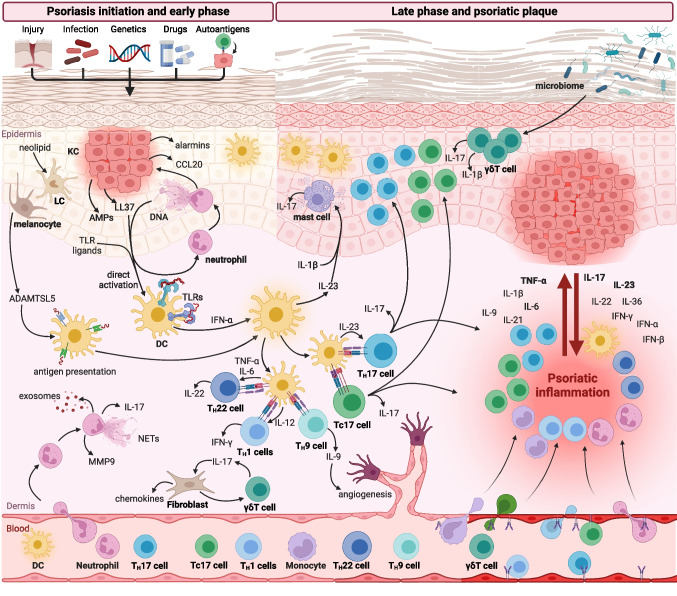
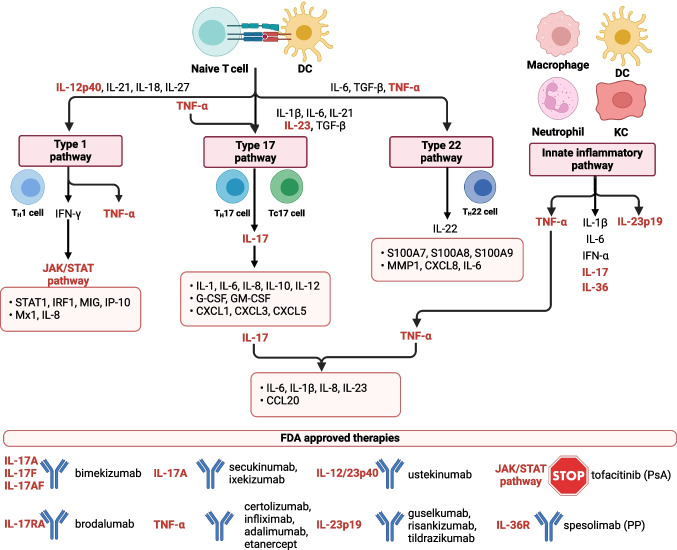
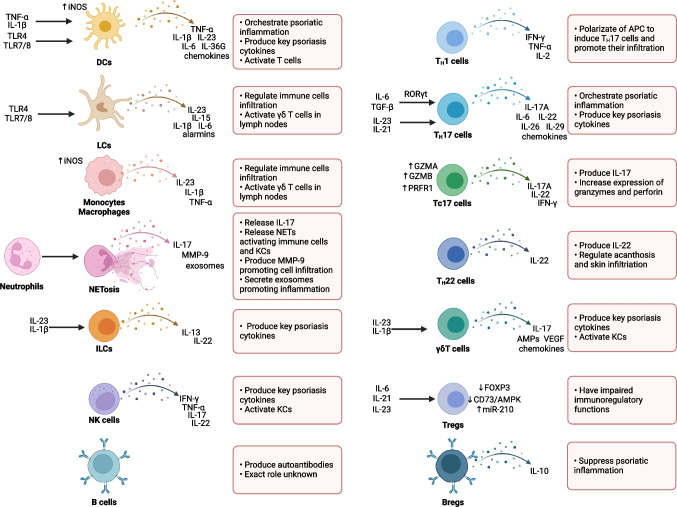
Psoriasis is one of the most common inflammatory skin diseases with a chronic, relapsing-remitting course. The last decades of intense research uncovered a pathological network of interactions between immune cells and other types of cells in the pathogenesis of psoriasis. Emerging evidence indicates that dendritic cells, TH17 cells, and keratinocytes constitute a pathogenic triad in psoriasis. Dendritic cells produce TNF-α and IL-23 to promote T cell differentiation toward TH17 cells that produce key psoriatic cytokines IL-17, IFN-γ, and IL-22. Their activity results in skin inflammation and activation and hyperproliferation of keratinocytes. In addition, other cells and signaling pathways are implicated in the pathogenesis of psoriasis, including TH9 cells, TH22 cells, CD8+ cytotoxic cells, neutrophils, γδ T cells, and cytokines and chemokines secreted by them. New insights from high-throughput analysis of lesional skin identified novel signaling pathways and cell populations involved in the pathogenesis. These studies not only expanded our knowledge about the mechanisms of immune response and the pathogenesis of psoriasis but also resulted in a revolution in the clinical management of patients with psoriasis. Thus, understanding the mechanisms of immune response in psoriatic inflammation is crucial for further studies, the development of novel therapeutic strategies, and the clinical management of psoriasis patients. The aim of the review was to comprehensively present the dysregulation of immune response in psoriasis with an emphasis on recent findings. Here, we described the role of immune cells, including T cells, B cells, dendritic cells, neutrophils, monocytes, mast cells, and innate lymphoid cells (ILCs), as well as non-immune cells, including keratinocytes, fibroblasts, endothelial cells, and platelets in the initiation, development, and progression of psoriasis.
Keywords: Immune response; Keratinocyte; Psoriasis; Skin inflammation; TH17 cells.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
