

A case of methotrexate-related lymphoproliferative disease showing multiple liver lesions in a patient with rheumatoid arthritis
- PMID: 38642276
- PMCID: PMC11284183
- DOI: 10.1007/s12328-024-01963-6
A case of methotrexate-related lymphoproliferative disease showing multiple liver lesions in a patient with rheumatoid arthritis
Abstract
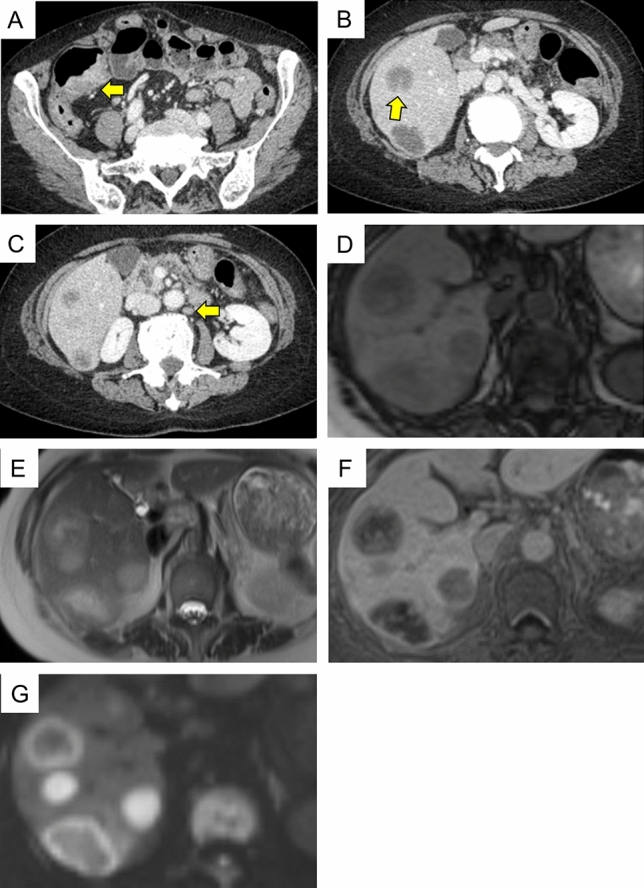
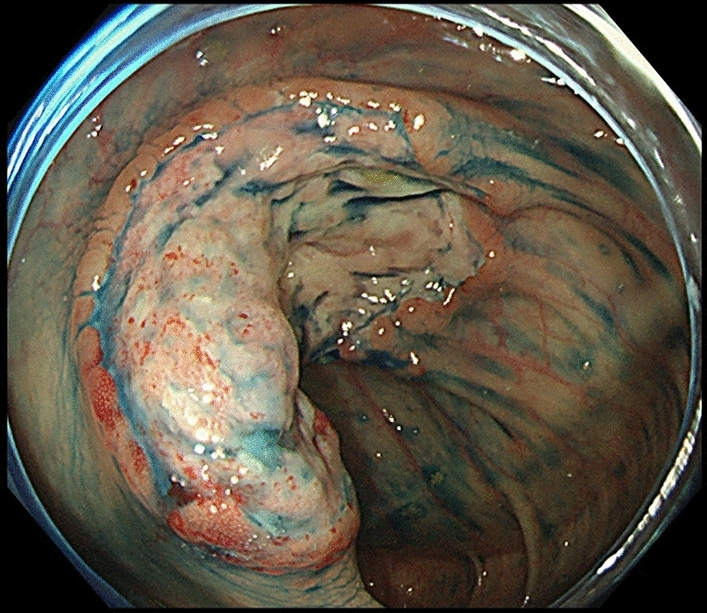
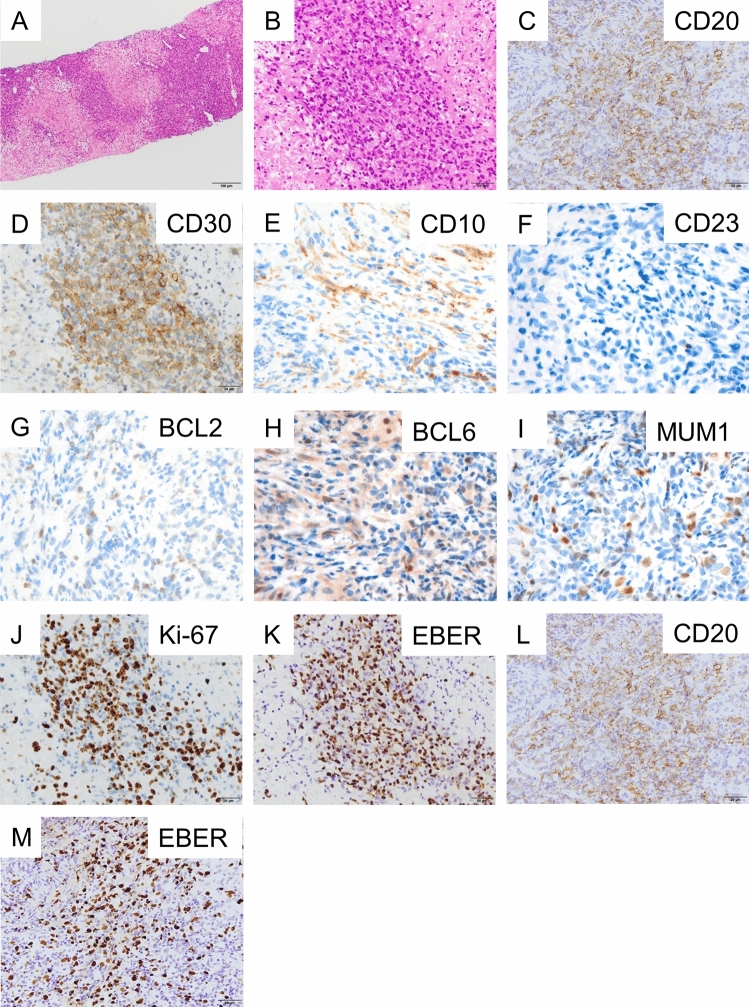
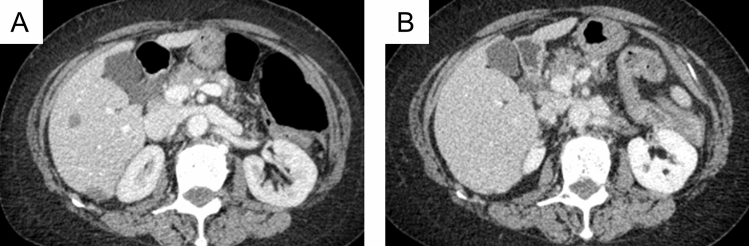
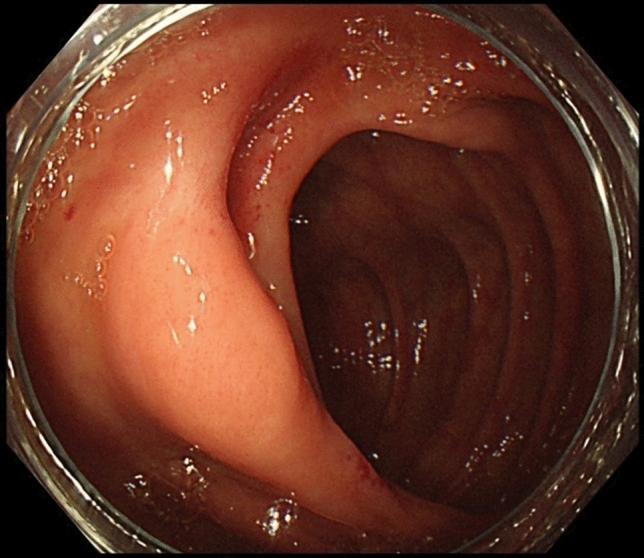
A 66-year-old woman with rheumatoid arthritis (RA) who had been receiving methotrexate (MTX) for 2 years presented with tarry stools. Contrast-enhanced computed tomography (CT) of the abdomen revealed irregular wall thickening in the ileocecal region and multiple low-contrast masses in both lobes of the liver. Lower gastrointestinal endoscopy revealed a type 2 tumor in the ileocecal region with a semi-peripheral ulcer. Histological examination of liver and colon biopsies showed other iatrogenic immunodeficiency-associated lymphoproliferative disorder (Oi-LPD), diffuse large B-cell lymphoma type, with positivity for Epstein-Barr virus DNA. After withdrawal of MTX, the LPD lesions disappeared and the patient achieved remission. We considered this to be a sporadic case of Oi-LPD, diffuse large B-cell lymphoma type, in the liver and colon due to treatment with MTX. There has been no previous report of this condition with simultaneous hepatic and colonic lesions, and the present case is thought to be highly informative in relation to the pathogenesis.
Keywords: Colon; Diffuse large B-cell lymphoma; Liver; Methotrexate-related lymphoproliferative disease; Rheumatoid arthritis.
© 2024. The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
A case of multiple hepatic lesions associated with methotrexate-associated lymphoproliferative disorder.J Med Ultrason (2001). 2016 Oct;43(4):545-51. doi: 10.1007/s10396-016-0740-y. Epub 2016 Aug 30. J Med Ultrason (2001). 2016. PMID: 27577564
-
Methotrexate-related lymphoproliferative disorder of the stomach in a patient with rheumatoid arthritis: a case of disease regression after methotrexate cessation.Clin J Gastroenterol. 2016 Feb;9(1):17-21. doi: 10.1007/s12328-015-0624-5. Epub 2016 Jan 5. Clin J Gastroenterol. 2016. PMID: 26733461 Free PMC article.
-
[Primary central nervous system methotrexate associated lymphoproliferative disorders in a patient with rheumatoid arthritis].Rinsho Shinkeigaku. 2018 Aug 31;58(8):485-491. doi: 10.5692/clinicalneurol.cn-001157. Epub 2018 Jul 31. Rinsho Shinkeigaku. 2018. PMID: 30068810 Japanese.
-
Spontaneous regression of breast lymphoproliferative disorders after withdrawal of methotrexate in rheumatoid arthritis patients with Epstein-Barr virus infection: a case report and review of the literature.J Med Case Rep. 2022 Feb 7;16(1):49. doi: 10.1186/s13256-022-03274-1. J Med Case Rep. 2022. PMID: 35125110 Free PMC article. Review.
-
Lymphoproliferative disorders in patients with rheumatoid arthritis in the era of widespread use of methotrexate: A review of the literature and current perspective.Mod Rheumatol. 2018 Jan;28(1):1-8. doi: 10.1080/14397595.2017.1352477. Epub 2017 Jul 31. Mod Rheumatol. 2018. PMID: 28758827 Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
